End-of-life care for patients with advanced lung cancer and chronic obstructive pulmonary disease: survey among Polish pulmonologists
Key words: advanced chronic obstructive pulmonary disease, breathlessness, end-of-life communication, opioids, palliative care



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
End-of-life care for patients with advanced lung cancer and chronic obstructive pulmonary disease: survey among Polish pulmonologists
Introduction: There is evidence that people with nonmalignant disease receive poorer end‑of‑life (EOL) care compared with people with cancer.
Objectives: The aim of the study was to assess the selected aspects of symptomatic treatment and communication between physicians and patients diagnosed with either advanced chronic obstructive pulmonary disease (COPD) or lung cancer.
Methods: A questionnaire survey was conducted online among members of the Polish Respiratory Society.
Results: Properly completed questionnaires were returned by 174 respondents (27.2% of those proved to be contacted by email). In COPD, 32% of respondents always or often used opioids in chronic breathlessness and 18.3% always or often referred patients to a palliative care (PC) specialist. Nearly 80% of the respondents claimed that bedside discussions on EOL issues with people with COPD are essential, although only 20% would always or often initiate them. In people with lung cancer, opioids were routinely used for relief of chronic breathlessness by 80% of physicians; 81.7% referred patients to a PC specialist. More than half of the respondents always or often discussed EOL issues only with the patient’s caregivers or relatives. Younger physicians, those at an earlier stage of their career, those caring for higher numbers of patients with lung cancer, and those who were better acquainted with Polish Respiratory Society recommendations for PC in chronic lung diseases seemed to provide better EOL care for COPD patients.
Conclusions: Patients with COPD, as compared with patients with lung cancer, were less frequently treated with opioids to relieve chronic breathlessness or referred for a PC consultation. Discussing the EOL issues with a patient was generally found challenging by physicians, and most often pursued with caregivers instead. The COPD recommendations on PC may prove helpful in providing better EOL care by pulmonologists.
Introduction
A steadily rising number of patients diagnosed with chronic obstructive pulmonary disease (COPD), especially those at an advanced stage of the disease, has triggered an ongoing debate over palliative care (PC) for this particular group of patients. Numerous studies revealed the burden of ineffectively controlled symptoms such as chronic breathlessness, depression, and anxiety among patients with end‑stage COPD.1-3 Compared with other life‑limiting conditions, these patients experience lower quality of life, and yet they have limited access to PC or even a PC consultation.4-6 There is also evidence of ineffective communication between pulmonologists and people with COPD, especially on end‑of‑life (EOL) issues.7-9 Patients usually expect their physicians to be able to explain to them the key aspects of their condition, including future care needs. On the other hand, patients usually do not initiate conversations about EOL issues themselves during a consultation.10,11 Recently, international and local recommendations for PC in advanced nonmalignant lung diseases have been introduced, including guidelines of the Polish Respiratory Society (PRS).12-16
We carried out a questionnaire survey among Polish pulmonologists 5 years after the publication of the Polish guidelines, with the aim to assess their understanding and uptake of specific recommendations in everyday clinical practice. We aimed to compare how attending pulmonary physicians treated symptoms and communicated with patients with advanced COPD and those with lung cancer. The comparison between COPD and lung cancer seems to be relevant since both conditions are characterized by common pathogenesis,17 similar presentation, and comparable prognosis at their advanced stage.
Methods
The online questionnaire was developed for the purpose of this research, based on a tool used in a Portuguese study by Gaspar et al,18 but expanded to 2 patient populations, namely, those with advanced COPD and those with lung cancer. The questionnaire was divided into 5 thematic domains: symptom management, EOL communication, participants in EOL communication, obstacles to EOL communication, and a sense of dignity in a COPD patient.
With regard to the first 3 domains, a Likert scale was used to elicit respondents’ opinions (1 – never; 2 – seldom; 3 – occasionally; 4 – often; and 5 – always). In the “obstacles to communication” category, respondents were asked to mark as many options as they deemed essential. Finally, there was an open question on how to support dignity in a patient with COPD at the end of life.
The questionnaire was loaded onto the Survio survey platform (https://www.survio.com). All members of the PRS who were also physicians were sent an email with an invitation to complete the questionnaire anonymously, and a reminder was sent 3 times within 4 months.
The study protocol was approved by the Bioethics Review Committee at Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Poland (Ref. No. KB 667/2016).
Statistical analysis
The differences in the results between people with COPD and lung cancer measured on the ordinal scale were tested using the Mann–Whitney test. Nominal variables were assessed with the χ2 independence test. Correlations between the variables were established with the Kendall’s τ-b correlation coefficient. The level of statistical significance was set at a P value of less than 0.01. The SPSS software (IBM SPSS Statistics 24.0.0; SPSS Inc., Armonk, New York, United States) was used for analyses.
Results
Study participants
An invitation to participate in the study was sent to 958 email addresses from the database of the PRS; however, only 639 respondents were contactable by email (Supplementary material, Figure S1). A total of 176 members of the PRS completed the survey; however, 2 questionnaires were excluded from the analysis due to critical technical errors. Finally, 174 correctly completed questionnaires were received, yielding a response rate of 27.2% (174 of 639). The average age of respondents was 49 years (range, 28–86 years; Table 1) and 59% of respondents were women. Most people worked in the profession for over 10 years, and nearly 90% of respondents held a specialization in pulmonology. For 29% of respondents, the main place of work was a university hospital, and for 43%, another type of hospital. The majority of respondents (88%) treated more than 50 people with COPD within a year, with 70% caring for 30 or more people with category D according to the Global Initiative for Chronic Obstructive Lung Disease classification in the preceding year.19 More than half of respondents (56%) cared for at least 50 people with lung cancer within a year. Most of the pulmonologists who participated in the study were aware of the PRS guidelines on PC in chronic lung diseases: 40% of respondents had read them and 36% briefly reviewed them.
Age, mean (SD) | 49.2 (11) | |
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: COPD, chronic obstructive pulmonary disease; PC, palliative care; PRS, Polish Respiratory Society | ||
Female sex | 102 (58.6) | |
Years of practice | <5 years | 6 (3) |
5–9 years | 9 (5) | |
10–19 years | 48 (28) | |
20–29 years | 66 (38) | |
>30 years | 45 (26) | |
Specialty held | Respiratory medicine | 156 (90) |
Allergology | 21 (12) | |
Palliative medicine | 5 (3) | |
The main place of work | University hospital | 50 (29) |
Another hospital | 75 (43) | |
Outpatient clinic | 32 (18) | |
Private practice | 10 (6) | |
Number of COPD patients treated within a year | <50 | 21 (12) |
50–200 | 81 (47) | |
>200 | 72 (41) | |
Number of lung cancer patients treated within a year | <50 | 76 (44) |
50–200 | 80 (46) | |
>200 | 18 (10) | |
Number of category D patients with COPD treated during last year | <30 | 52 (30) |
30–100 | 90 (52) | |
>100 | 52 (18) | |
Knowledge of PRS guidelines on PC in lung diseases | I know them and I have read them. | 70 (40.2) |
I have heard about them and looked through them briefly. | 63 (36.2) | |
I have heard about them, but not read them. | 18 (10.3) | |
I have never heard of them. | 23 (13.2) | |
Religious beliefs | Christian | 135 (77.6) |
Nonbeliever | 21 (12.1) | |
Buddhist | 0 | |
Muslim | 0 | |
Other | 1 (1.7) | |
I prefer not to answer. | 15 (8.6) | |
Relief of symptoms
As to relieving moderate or severe pain, opioids were more often used in patients with advanced lung cancer than in those with COPD (always or often, 86.8% and 28.2%, respectively; Table 2). As to relieving chronic breathlessness20 in people with advanced lung cancer, opioids were used significantly more often than in advanced COPD (always or often, 79.4% and 32.2%, respectively). For people with COPD, the majority of physicians used opioids only occasionally (31.6%), or seldom or never (36%; Table 2).
Lung cancer | COPD | P value | z score | ||
Data are presented as number (percentage) unless otherwise stated.
Abbreviations: NS, nonsignificant; others, see Table 1 | |||||
Frequency of opioid use in relieving severe to moderate pain in patients with advanced stages of the disease | 1 – never | 7 (4) | 33 (19) | <0.001 | –11.69 |
2 – seldom | 0 | 33 (19) | |||
3 – occasionally | 16 (9.2) | 59 (33.9) | |||
4 – often | 63 (36.2) | 41 (23.6) | |||
5 – always | 88 (50.6) | 8 (4.6) | |||
Median | 5 | 3 | |||
Frequency of opioid use in relieving chronic breathlessness in patients with advanced stages of the disease | 1 – never | 9 (5.2) | 29 (16.7) | <0.001 | –9.11 |
2 – seldom | 9 (5.2) | 34 (19.5) | |||
3 – occasionally | 18 (10.3) | 55 (31.6) | |||
4 – often | 69 (39.7) | 44 (25.3) | |||
5 – always | 69 (39.7) | 12 (6.9) | |||
Median | 4 | 3 | |||
Frequency of concerns regarding opioid use in patients with chronic breathlessness in advanced stages of the disease | 1 – never | 102 (62) | 31 (17.8) | <0.001 | –9.27 |
2 – seldom | 47 (27) | 60 (34.5) | |||
3 – occasionally | 14 (8) | 43 (24.7) | |||
4 – often | 4 (2.3) | 28 (16.1) | |||
5 – always | 1 (0.6) | 12 (6.9) | |||
Median | 1 | 2 | |||
Frequency of favorable effects of opioid use in COPD patients with chronic breathlessness | 1 – never | – | 12 (6.9) | – | – |
2 – seldom | – | 11 (6.3) | |||
3 – occasionally | – | 37 (21.3) | |||
4 – often | – | 95 (54.6) | |||
5 – always | – | 19 (10.9) | |||
Median | – | 4 | |||
Frequency of recommending antidepressant or anxiolytic therapy in patients with depression or anxiety disorders in advanced stages of the disease | 1 – never | 1 (0.6) | 1 (0.6) | NS | –1.67 |
2 – seldom | 16 (9.2) | 27 (15.5) | |||
3 – occasionally | 59 (33.9) | 58 (33.3) | |||
4 – often | 74 (42.5) | 72 (41.4) | |||
5 – always | 24 (13.8) | 16 (9.2) | |||
Median | 4 | 4 | |||
The majority of study participants who used opioids to relieve chronic breathlessness in patients with COPD often or always noticed benefits (65.5%). More physicians never had any concerns that would made them reluctant to use opioids in chronic breathlessness while treating patients with lung cancer as compared with patients with COPD (62% and 17.8%, respectively).
Among 96 answers (given by 82 participants) to the open question about the fears connected with using opioids, the majority were related to the risk of respiratory depression (n = 56) and the balance with adverse effects such as constipation, nausea, or drowsiness (n = 12), and the potential for serious complications such as consciousness disturbances (n = 6) or development of opioid addiction (n = 4).
The correlation analysis revealed a significant relationship between the frequency of using opioids to relieve pain and chronic breathlessness and the following factors: age, work experience, number of people with lung cancer treated within a year, and knowledge of the PRS guidelines for PC in lung diseases (Table 3).
Variables | Test | Frequency of opioid use in relieving severe or moderate pain | Frequency of opioid use in relieving chronic breathlessness | Frequency of recommending antidepressant or anxiolytic | Frequency of favorable effects of opioids in COPD patients with chronic breathlessness | Frequency of concerns regarding opioid use | ||||
Lung cancer | COPD | Lung cancer | COPD | Lung cancer | COPD | Lung cancer | COPD | |||
a The Kendall’s τ-b correlation coefficient was applied.
b The Mann–Whitney test was applied.
| ||||||||||
Agea | Coefficient | –0.12 | –0.24 | –0.17 | –0.21 | –0.04 | –0.08 | –0.21 | 0.13 | 0.10 |
Significance | NS | <0.001 | 0.005 | <0.001 | NS | NS | <0.001 | NS | NS | |
Sexb | Test value | –0.35 | –1.29 | –0.19 | –0.17 | –0.58 | –0.60 | –1.06 | –0.69 | –1.46 |
Significance | NS | NS | NS | NS | NS | NS | NS | NS | NS | |
Work experiencea | Coefficient | –0.09 | –0.22 | –0.14 | –0.21 | –0.03 | –0.09 | –0.23 | 0.13 | 0.12 |
Significance | NS | <0.001 | NS | 0.001 | NS | NS | <0.001 | NS | NS | |
Number of COPD patients treated within a yeara | Coefficient | – 0.02 | –0.02 | –0.06 | –0.01 | 0.01 | 0.08 | 0.04 | 0.07 | –0.03 |
Significance | NS | NS | NS | NS | NS | NS | NS | NS | NS | |
Number of lung cancer patients treated within a yeara | Coefficient | 0.10 | 0.22 | 0.22 | 0.21 | 0.26 | 0.28 | 0.14 | –0.02 | –0.03 |
Significance | NS | 0.001 | 0.001 | 0.001 | <0.001 | <0.001 | NS | NS | NS | |
Knowledge of PRS guidelinesa | Coefficient | –0.20 | –0.22 | –0.21 | –0.23 | –0.20 | –0.17 | –0.18 | 0.01 | 0.17 |
Significance | 0.004 | 0.001 | 0.001 | <0.001 | 0.003 | NS | 0.007 | NS | 0.008 | |
Religious beliefs (believer or nonbeliever)b | Value of test | –0.97 | –1.15 | –0.94 | –0.31 | –0.78 | –0.33 | –0.61 | –0.53 | –0.24 |
Significance | NS | NS | NS | NS | NS | NS | NS | NS | NS | |
Study participants who had better knowledge of the PRS guidelines were more likely to use opioids for pain and chronic breathlessness in both groups of patients. Younger respondents and those treating higher numbers of patients with lung cancer were more open to the use of opioids to manage pain in people with COPD and to reduce chronic breathlessness in both patient groups.
Study participants who were at earlier stages of their career were more likely to use opioids for pain and chronic breathlessness in people with COPD. Younger pulmonologists, those earlier in their career, and those with a better knowledge of the PRS guidelines were also more open to see favorable effects of opioids in patients with COPD and chronic breathlessness. A significant relationship was revealed between the frequency of concerns about the use of opioids in patients with COPD and lower familiarity with the PRS guidelines for PC in lung disease.
No significant difference was observed in the pulmonologists’ attitude to the treatment of mood disorders in patients with COPD and lung cancer (Table 2). Prescribing antidepressants and anxiolytics in both groups of patients was correlated with the number of people with lung cancer treated within a year (Table 3). A significant relationship was also revealed between the frequency of recommending antidepressants and anxiolytics in patients with lung cancer and good knowledge of the PRS guidelines.
End‑of‑life communication
Most of the respondents believed that discussions about the EOL issues with patients with COPD were essential (79%; Table 4), yet only 20% of respondents often or always initiated these conversations. Slightly more physicians initiated such conversations with patients with lung cancer (always or often, 39.1%).
Lung cancer | COPD | P value | z score | ||
Frequency of talks with patients on the subject of: | |||||
Frequency of making a suggestion to the patient that a decision needs to be made on: | |||||
Lung cancer | COPD | P value | z score | ||
Data are presented as number (percentage) unless otherwise stated.
| |||||
Frequency of initiating a talk with patients regarding EOL issues | 1 – never | 22 (12.6) | 26 (14.9) | 0.001 | –3.40 |
2 – seldom | 42 (24.1) | 64 (36.8) | |||
3 – occasionally | 42 (24.1) | 49 (28.2) | |||
4 – often | 49 (28.2) | 27 (15.5) | |||
5 – always | 19 (10.9) | 8 (4.6) | |||
Median | 3 | 2 | |||
Disease progression | 1 – never | 0 | 0 | NS | –1.92 |
2 – seldom | 15 (8.6) | 10 (5.7) | |||
3 – occasionally | 39 (22.4) | 25 (13.2) | |||
4 – often | 74 (42.5) | 89 (51.1) | |||
5 – always | 46 (26.4) | 52 (29.9) | |||
Median | 4 | 4 | |||
Everyday needs | 1 – never | 1 (0.6) | 3 (1.7) | NS | –0.31 |
2 – seldom | 22 (12.6) | 18 (10.3) | |||
3 – occasionally | 44 (25.3) | 42 (24.1) | |||
4 – often | 63 (36.2) | 77 (44.3) | |||
5 – always | 44 (25.3) | 34 (19.5) | |||
Median | 4 | 4 | |||
End‑of‑life symptoms | 1 – never | 18 (10.3) | 24 (13.8) | 0.004 | –2.90 |
2 – seldom | 43 (24.7) | 57 (32.8) | |||
3 – occasionally | 45 (25.9) | 52 (29.9) | |||
4 – often | 49 (28.2) | 31 (17.8) | |||
5 – always | 19 (10.9) | 10 (5.7) | |||
Median | 3 | 3 | |||
Religious/spiritual needs | 1 – never | 42 (24.1) | 50 (28.7) | NS | –2.23 |
2 – seldom | 50 (28.7) | 64 (36.8) | |||
3 – occasionally | 38 (21.8) | 32 (18.4) | |||
4 – often | 29 (16.7) | 20 (11.5) | |||
5 – always | 15 (8.6) | 8 (4.6) | |||
Median | 2 | 2 | |||
Invasive mechanical ventilation | 1 – never | 75 (43.1) | 21 (12.1) | <0.001 | –7.13 |
2 – seldom | 47 (27) | 37 (21.3) | |||
3 – occasionally | 26 (14.9) | 54 (31) | |||
4 – often | 19 (10.9) | 50 (28.7) | |||
5 – always | 7 (4) | 12 (6.9) | |||
Median | 2 | 3 | |||
Cardiopulmonary resuscitation | 1 – never | 85 (48.9) | 42 (24.1) | <0.001 | –4.77 |
2 – seldom | 53 (30.5) | 59 (33.9) | |||
3 – occasionally | 17 (9.8) | 51 (29.3) | |||
4 – often | 12 (6.9) | 19 (10.9) | |||
5 – always | 7 (4) | 3 (1.7) | |||
Median | 2 | 2 | |||
Place of dying | 1 – never | 42 (24.1) | 65 (37.4) | <0.001 | –3.87 |
2 – seldom | 46 (26.4) | 56 (32.2) | |||
3 – occasionally | 38 (21.8) | 30 (17.2) | |||
4 – often | 34 (19.5) | 18 (10.3) | |||
5 – always | 14 (8) | 5 (2.9) | |||
Median | 2 | 2 | |||
Frequency of referring a patient for PC or to a palliative medicine specialist | 1 – never | 8 (4.6) | 42 (24.1) | <0.001 | –11.41 |
2 – seldom | 8 (4.6) | 51 (29.3) | |||
3 – occasionally | 16 (9.2) | 49 (28.2) | |||
4 – often | 81 (46.6) | 26 (14.9) | |||
5 – always | 61 (35.1) | 6 (3.4) | |||
Median | 4 | 2 | |||
Whether the discussions on EOL with an advanced COPD patient are needed and important for the patient | They are needed and important | – | 137 (78.7) | – | – |
They are neither needed nor important | – | 5 (2.9) | |||
I have no opinion | – | 32 (18.4) | |||
With regards to patients with advanced COPD, the most frequently discussed topics were disease progression (81% of respondents discussed it always or often) and everyday needs (always or often, 63.8%). Discussion on the EOL symptoms were much less frequent (always or often, 23.5%), similarly to talks on religious or spiritual needs (always or often, 16.1%; Table 4). The same topics were also most frequently addressed in people with lung cancer. Mechanical ventilation was always or often discussed with people who had COPD by 35.6% of respondents. Patients with lung cancer were significantly less likely to have a discussion about mechanical ventilation (15%; Table 4). Only 12.6% of respondents discussed cardiopulmonary resuscitation with patients with COPD, and 10.9% with patients with advanced lung cancer. Conversations about the place of dying were rare in both patient populations. A higher number of people with COPD and lung cancer treated within a year positively influenced the initiation of EOL discussion by physicians (Table 5). A better knowledge of the PRS guidelines was related to more frequent initiation of a discussion on EOL issues with patients with COPD.
Variable | Test | Frequency of initiating a talk on EOL issues | Frequency of suggesting to a patient at an advanced stage of the disease the need for making a decision regarding: | ||||||
Invasive mechanical ventilation | Cardiopulmonary resuscitation | Place of dying | |||||||
a The Kendall τ-b correlation coefficient was applied.
b The Mann–Whitney test was applied.
Abbreviations: see Tables 1, 2, and 4 | |||||||||
Lung cancer | COPD | Lung cancer | COPD | Lung cancer | COPD | Lung cancer | COPD | ||
Agea | Correlation coefficient | –0.10 | –0.09 | 0.01 | 0.11 | 0.04 | 0.00 | –0.20 | –0.14 |
Significance | NS | NS | NS | NS | NS | NS | <0.001 | NS | |
Sexb | Test value | –1.47 | –1.07 | –0.64 | –0.46 | –0.44 | –1.24 | –0.36 | –0.35 |
Significance | NS | NS | NS | NS | NS | NS | NS | NS | |
Work experiencea | Correlation coefficient | –0.10 | –0.10 | 0.04 | 0.10 | 0.02 | 0.00 | –0.21 | –0.14 |
Significance | NS | NS | NS | NS | NS | NS | 0.001 | NS | |
Number of COPD patients treated within a yeara | Correlation coefficient | 0.18 | 0.18 | 0.13 | 0.25 | 0.08 | 0.10 | 0.12 | 0.11 |
Significance | 0.006 | 0.007 | NS | <0.001 | NS | NS | NS | NS | |
Number of lung cancer patients treated within a yeara | Correlation coefficient | 0.18 | 0.24 | – 0.04 | 0.10 | 0.05 | 0.13 | 0.20 | 0.19 |
Significance | 0.005 | <0.001 | NS | NS | NS | NS | 0.003 | 0.005 | |
Knowledge of Polish guidelinesa | Correlation coefficient | –0.16 | –0.21 | –0.09 | –0.25 | 0.07 | –0.30 | –0.10 | –0.07 |
Significance | NS | 0.001 | NS | <0.001 | NS | <0.001 | NS | NS | |
Religious beliefs (believer or nonbeliever)b | Test value | –1.87 | –0.72 | –0.06 | –0.66 | –0.50 | –0.45 | –1.00 | –1.37 |
Significance | NS | NS | NS | NS | NS | NS | NS | NS | |
Pulmonologists who treated higher numbers of people with lung cancer were more inclined to initiate bedside discussions about the preferred place of dying with both patient groups (Table 5). Younger physicians and those earlier in their careers were more open to discuss this topic with people who had lung cancer. Physicians who cared for a higher number of people with COPD were more inclined to suggest to a patient with COPD the need for making a decision regarding invasive mechanical ventilation. Better knowledge of the guidelines was associated with more frequent initiation of discussion on the use of invasive ventilation and cardiopulmonary resuscitation with COPD patients (Table 5).
Referral to specialist palliative care
People with lung cancer were more often referred for PC or a consultation with a palliative medicine specialist, with 81.7% of respondents always or often doing this. As to patients with COPD, only 18.3% of respondents (always or often) referred them for PC (Table 4).
Participants in end‑of‑life communication
More than half of the respondents (often or always) discussed the EOL issues with the caregivers or the patient’s family only, with the patient being excluded from the conversation (54%; Table 6). On the other hand, only 8.6% of respondents always or often made the decisions regarding the EOL of patients with COPD along with other health care specialists without including patients or their caregivers or relatives.
1 – never | 2 – seldom | 3 – occasionally | 4 – often | 5 – always | Median | |
Data are presented as number (percentage) unless otherwise stated.
| ||||||
Frequency of EOL discussions with the caregivers or relatives only, without the patient’s participation | 7 (4) | 27 (15.5) | 46 (26.4) | 71 (40.8) | 23 (13.2) | 4 |
Frequency of decisions on EOL issues regarding patients with end‑stage COPD made by the respondent, along with other specialists, without including patients or their caregivers or relatives | 47 (27) | 64 (36.8) | 48 (27.6) | 14 (8) | 1 (0.6) | 2 |
Obstacles to end‑of‑life communication
The following key obstacles to initiating talks about the EOL issues with a patient who has end‑stage COPD were identified: belief that a patient was not ready for such talk (68.4%); fear of stripping the patient of hope (64.9%); lack of the resources necessary to provide PC for the patient (49.4%); and certain inadequacies in training in this particular area (33.9%). More than 20% of respondents pointed to lack of clarity regarding the legal aspects of making medical decisions at the end of the patient’s life (23.6%) and to difficulties in predicting the actual progression of the disease (20.1%; Figure 1).
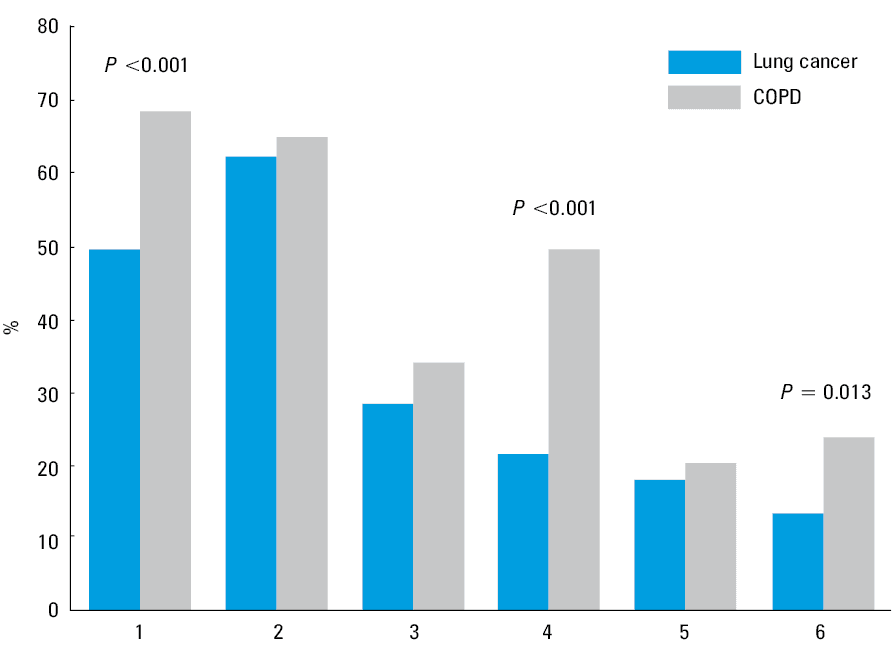
Similar obstacles were identified for people with lung cancer: fear of stripping hope (62.1%); belief that a patient was not ready for such discussion (49.4%); inadequate training (28.2%); lack of the resources necessary to provide PC for the patient (21.3%); difficulties in predicting the actual progression rate of the disease (17.8%); and ignorance of pertinent legal aspects (13.2%; Figure 1).
More respondents recognized obstacles hampering communication on EOL issues in people with COPD than lung cancer: the impression that patients are unprepared for facing such issues (68.4% and 49.4%, respectively) and lack of the resources necessary to provide PC for a patient (49.4% and 21.3%, respectively).
Dignity in patients with chronic obstructive pulmonary disease
Finally, an open question was posed on how to effectively enhance dignity in people with COPD approaching the end of life. We received 108 answers, and the need for better access to PC centers or home PC was highlighted most often (n = 24). There were also numerous suggestions for more person‑oriented treatment in terms of better sharing of information about the nature of their disease and encouraging their informed involvement in making pertinent therapeutic decisions (n = 15). Respondents also highlighted the importance of caring for patients’ families (n = 14), better access to psychological services (n = 13), and more empathy from attending physicians (n = 8).
Discussion
Caring for people with advanced chronic obstructive pulmonary disease
Despite Polish and other guidelines on COPD that recommend PC approach including efficient management of symptoms and advance care planning,12-16,19,21,22 chronic breathlessness remains undertreated, physicians rarely initiate discussions on EOL issues and seldom refer their patients to a PC specialist.18,23-26 A total of 19% of respondents reported that they never prescribe opioids to people with chronic breathlessness and COPD, which is similar to the results from a study among Dutch chest physicians.24 Although the beneficial effects of opioids27-32 and their general safety (assuming that small, regular doses are prescribed) in relieving chronic breathlessness have been confirmed in various clinical trials,33-35 a significant percentage of the respondents still express serious reluctance to use them in practice. A similar attitude of pulmonologists was observed in a Portuguese study by Gaspar et al,18 in which 30% of respondents never or seldom used opioids in chronic breathlessness in patients with COPD.
In our survey, 1 in 4 participants always or often expressed concerns regarding opioids that make them reluctant to use those drugs in people with COPD and chronic breathlessness, which is consistent with other studies reporting that 15% to 56% of physicians were afraid of respiratory depression as an adverse effect of opioids in patients with COPD.24,36-38 A recent meta‑analysis showed no evidence of significant respiratory depression due to opioids used regularly at low doses for chronic breathlessness.35 Besides the lack of knowledge among physicians on when and how to use opioids, also preexisting fears contribute to doctors’ reluctance to prescribe opioids for chronic breathlessness, especially in COPD. Recently, we showed high incidence of opiophobia in Poland both among palliative care patients and physicians, creating an additional barrier to optimal treatment of chronic breathlessness.39,40 Half of Polish pulmonologists from the present study always or often prescribed antidepressant or anxiolytic therapy in people with advanced COPD experiencing depression or anxiety disorders, similarly to Portuguese study (60%).18 Further work is required to understand why 50% of pulmonologists did not.
Our survey revealed opportunities for better communication between pulmonologists and people with advanced COPD. Only 20% of respondents (always or often) initiated a discussion about EOL issues, which was comparable with results from a Portuguese study (13.2%).18 Few clinicians initiated such conversations including the topic of advance care planning. Clinicians avoided bringing up end‑of‑life symptoms, mechanical ventilation, or cardiopulmonary resuscitation. Respondents attributed barriers in an effective EOL approach to their belief that the patients were unprepared for facing such issues or that they did not want to destroy patients’ hopes.
A perceived lack of resources for providing PC for patients with COPD was also reported. A recent systematic review of studies on the practice of advance care planning among patients with chronic lung disease confirmed that it is uncommon, possibly due to the complex course of the disease and ambivalence of both patients and clinicians about engaging in these processes.41
Interestingly, in a recent multinational survey, nearly all pulmonologists and PC specialists from Australia, New Zealand, and United Kingdom participating in the study reported that they would initiate a discussion with the person described in a case vignette regarding prognosis and advance care planning.42 While physicians of both specialties pointed at similar topics that need to be covered in advance care planning, palliative medicine physicians were more likely to discuss death and dying issues, prognosis, treatment limitations, and the place of future care. Researchers proposed the complementarity of a pulmonologist and PC specialist, in which the former should initiate these discussions and the latter then develop and expand the conversations according to each patient’s needs and wishes, as the illness progresses.42 The cooperation between respiratory medicine and PC has been recommended by international guidelines, which pointed at early implementation of the PC approach in parallel with disease‑directed therapy.15,19 The ideal model should be based on good cooperation between the pulmonologist and PC specialist as well as an easy access to PC care for COPD patients. There is also a steadily growing body of evidence for the benefits offered by PC, even in the early stages of the disease.43 However, in the majority of countries referral to PC specialist services is still rare.44,45 In the United States, only 1.7% of patients with end‑stage COPD who were dependent on home oxygen were referred to a PC specialist when admitted with an exacerbation.45 In Poland there are no legal restrictions on access to PC by patients with advanced COPD. However, there are no models of care for advanced COPD patients apart from a few pilot programs such as the Integrated Care Model developed in Gdańsk, Poland.46,47
Better end‑of‑life care for patients with lung cancer than for those with chronic obstructive pulmonary disease
When compared with patients with advanced lung cancer, patients with advanced COPD are prescribed fewer opioids for the relief of moderate or severe pain and chronic breathlessness, and pulmonologists less often initiate bedside discussion on the EOL issues, refer them to PC, or ask PC specialist for consultation (Table 7). Concerns regarding the use of opioids, as expressed by physicians, were also more often related to patients with COPD, but such fears do not reflect the available evidence. Further, pulmonologists more often talk about EOL symptoms and initiate a discussion on the place of dying with patients with advanced lung cancer. Discussions about invasive mechanical ventilation and cardiopulmonary resuscitation are more frequent in people with advanced COPD, but even then are initiated only by a minority of physicians. Significantly more respondents recognized obstacles hampering communication on EOL issues in patients with COPD than with lung cancer, especially because of concerns that patients are unprepared for facing such issues and lack of the resources required to provide PC. Respondents highlighted the need to facilitate better access to PC centers and recognition of the patient’s rights to honest, factual information about their medical condition.
Selected aspects of treatment and communication; “often” or “always” responses | Disease | χ2 test | ||
COPD | Lung cancer | χ2 | P value | |
Data are presented as number (percentage).
Abbreviations: see Tables 1, 2, and 4 | ||||
Application of opioids for relieving moderate or severe pain | 49
(28) | 151
(87) | 122.32 | <0.001 |
Application of opioids for chronic breathlessness | 56
(32) | 138
(79) | 78.32 | <0.001 |
Concerns regarding the application of opioids in patients with chronic breathlessness | 40
(23) | 5
(3) | 31.27 | <0.001 |
Ordering antidepressant or anxiolytic treatment | 88
(51) | 98
(56) | 1.15 | NS |
Initiating a talk on EOL issues | 35
(20) | 68
(39) | 15.02 | <0.001 |
Referring a patient for PC or to a PC specialist consultation | 32
(18) | 142
(82) | 139.08 | <0.001 |
Why are people with COPD referred for PC less often? A recent population‑based survey from Belgium by Scheerens et al48 showed that treatment goals in the last week of life were less often aimed at comfort or palliation for COPD (59.1%) than for lung cancer (92.1%), and the use of any type of PC service was less common in COPD than in lung cancer (37.3% and 73.5%, respectively; P <0.001). In addition, the timing of referral was very close to death: a median of 6 days for COPD and 16 days for lung cancer. There is a need to define the indications for referral of patients with COPD for PC based on the level and complexity of needs and to demonstrate the benefits of early integration of PC into their care.49
Who should the doctor talk to about end‑of‑life issues?
More than half of the respondents (often or always) discussed EOL issues only with the caregivers or the patient’s family, with the patient being excluded from the conversation (54%). It is one of the most surprising results of this survey. In the Portuguese study,18 only 8.1% of respondents (often or always) had such conversations without the patient. Further studies should clarify whether respondents understood correctly that they were being asked about situations in which patients were still able to make their own decisions. If yes, then such physicians’ attitude to discuss EOL issues with the family or caregiver while excluding the most important person, the patient, needs to be carefully explored.
Professional factors related to care that was more aligned with the Polish Respiratory Society Guidelines
Four professional factors were significantly associated with the increased use of opioids. Respondents at a younger age and earlier in their career were more likely to use opioids to relieve chronic breathlessness in people with COPD and more frequently observed favorable effects of opioids in breathless patients with COPD. In a recent survey involving pulmonologists from Australia and New Zealand, a similar observation was made.36 It is probable that we are observing positive changes in a new generation of doctors, who are more open to the use of regular low‑dose morphine for symptom management.
A higher number of patients either with lung cancer or COPD treated within a year positively influenced the initiation of EOL talks by the physicians. The higher number in the COPD group was also related to the frequency of suggesting the need for making decision regarding invasive mechanical ventilation to a patient with COPD. However, caring for people with lung cancer also appears to be an important predictor of using opioids in patients with COPD and lung cancer to relieve chronic breathlessness. It may also predict ordering antidepressant or anxiolytic therapy in these patient populations and discussing the need for deciding on the place of dying. Caring for patients with cancer may make doctors more sensitive to the suffering of people with COPD, helping them not only to discuss EOL problems with patients, but also to introduce symptom management.
Better knowledge of the PRS guidelines was associated with the increased use of opioids in all patients, and the frequency of initiation of discussions on EOL issues and of addressing invasive ventilation and cardiopulmonary resuscitation in people with COPD. Respondents who did not know the PRS guidelines had concerns regarding the use of opioids in COPD patients more frequently. This observation seems to support the role of practice guidelines in improving the quality of patient care.
Limitations
The Polish Respiratory Society sent the invitation to participate in the research to all email addresses which had been collected in their database. Not knowing how many addresses were still active, we finally assumed the number of going to the website as a total number of doctors who received the invitation. The overall response rate is at the level expected for online surveys of professionals, reflecting results in similar studies.18,24,36 The survey assessed respondents’ self‑reported attitudes and knowledge, and thus might not reflect actual clinical practice in an objective way.
Conclusions
The results of this study highlight a great need to improve the procedures for relieving the symptoms and communicating more effectively with patients with advanced lung diseases. Palliative care standards for these patient groups should be more widely promoted, and a more compassionate, whole‑person care should be developed.50 Models of integrated care including partnership between pulmonologists and PC clinicians should especially address the unmet needs of patients with advanced COPD. It is of particular interest to find out whether the results of this survey are typical of Polish pulmonary physicians only, or perhaps indicative of a more universal phenomenon, so it would seem prudent to initiate a pan‑European research project in this area.
- Maddocks M, Lovell N, Booth S, et al. Palliative care and management of troublesome symptoms for people with chronic obstructive pulmonary disease (COPD). Lancet. 2017; 390: 988‑1002. | Crossref
- Górska L, Krajnik M, Damps‑Konstańska I, et al. Need for palliation in patients with the severe COPD ‑ a questionnaire study. Adv Palliat Med. 2007; 6: 107‑109.
- Yohannes AM, Kaplan A, Hanania NA. Anxiety and depression in Chronic Obstructive Pulmonary Disease: recognition and management. Cleve Clin J Med. 2018; 85 (suppl 1): S11‑S18. | Crossref
- Gore JM, Brophy CJ, Greenstone MA. How well we care for patients with end stage chronic obstructive pulmonary disease (COPD)? A comparison of palliative care and quality of life in COPD and lung cancer. Thora × 2000; 55: 1000‑1006. | Crossref
- Gavazzi A, De Maria R, Manzoli L, et al. Palliative needs for heart failure or chronic obstructive pulmonary disease: result of a multicenter observational registry. Int J Cardiol. 2015; 184: 552‑558. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION