Symptomatic metastatic pituitary lesions are a rare complication of the disseminated malignant neoplasia. The incidence of pituitary metastases is estimated at 0.87% of all intracranial ones.1 The most common are lung and breast cancer metastases, but kidney, thyroid, prostate, liver, and gastrointestinal cancer metastases to the pituitary have also been reported.2-5 Clinical symptoms occur in 2.5% to 18.2% cases only and typically include headaches, ophthalmoplegia, weakness, diabetes insipidus, and visual field defects.2
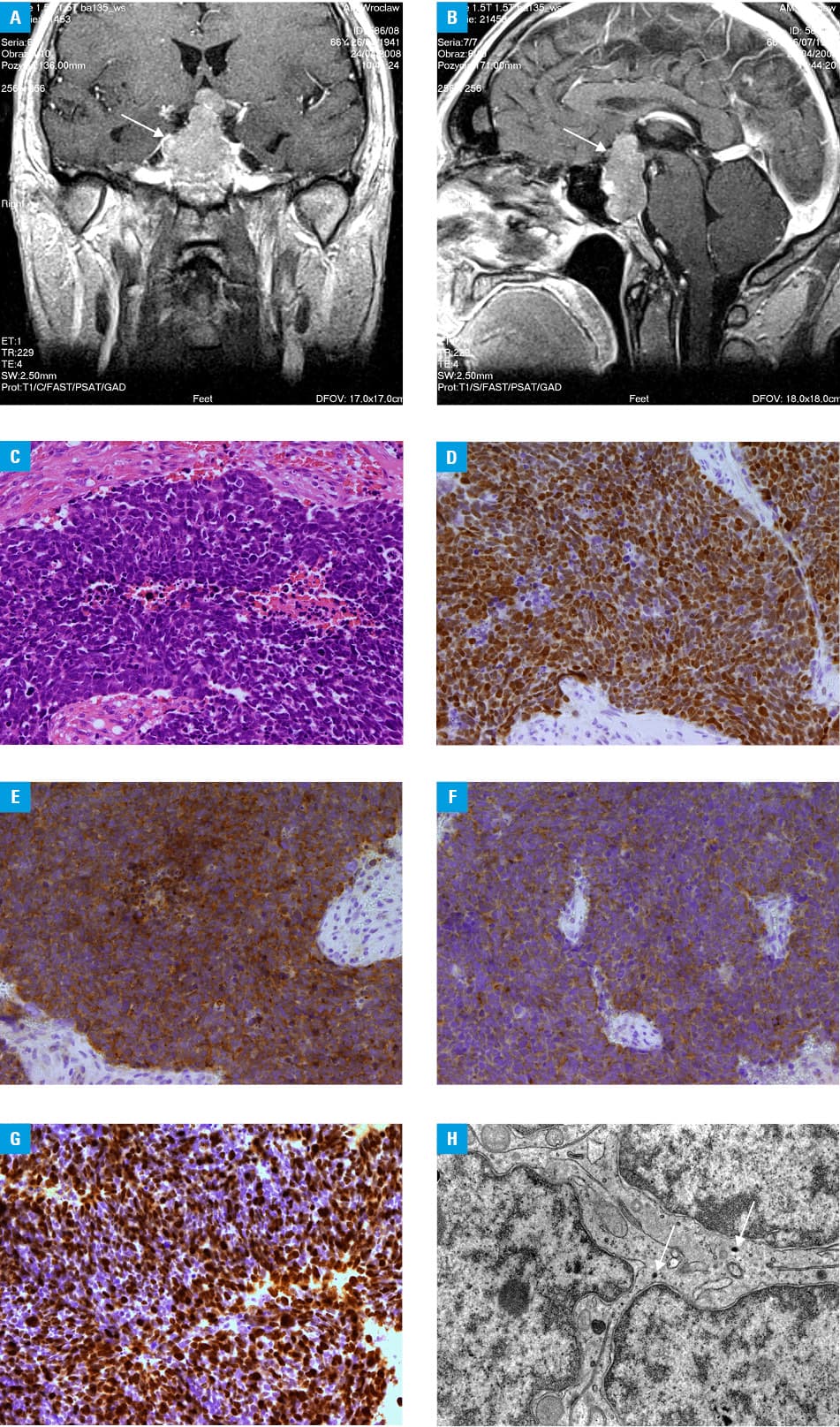
A 67‑year‑old man was referred to the endocrine department because of a large pituitary tumor, identified on computed tomography. The patient had reported a 4‑month history of fatigue, feeling of cold, blurred vision, and visual field defect. He denied headaches and diabetes insipidus symptoms. Computed tomography scans revealed a pituitary lesion (33 × 21 × 18 mm) causing local osteolysis and optic chiasm invasion. The patient reported a history of well‑controlled diabetes and hypertension, prostatectomy due to adenocarcinoma, eye cataract, and glaucoma. He was an active smoker at the time of examination. Hormonal evaluation revealed secondary hypothyroidism (thyroid stimulating hormone, 0.22 mIU/l; free triiodothyronine, 2.99 pmol/l; free thyroxine, 7.93 pmol/l), slightly increased prolactin level (38.5 ng/ml), hypogonadotropic hypogonadism (luteinizing hormone, 0.16 IU/l; follicle stimulating hormone, 1.01 IU/l; total testosterone, 0.2 ng/ml), secondary hypocortisolism (adrenocorticotropic hormone at 08:00 AM, 7.1 pg/ml; cortisol at 8:00 AM, 3.9 μg/dl), somatotropic insufficiency (growth hormone, 0.5 ng/ml; insulin‑like growth factor 1, 68 ng/ml). Serum osmolality was 288 mOsm/l, urine osmolality, 314 mOsm/l, and 24‑hour urine collection, 1350 ml. Ophthalmologic evaluation revealed bilateral temporal hemianopsia. The pituitary magnetic resonance imaging indicated a large tumor localized at intra- and extrasellar space, invading the cavernous sinus bilaterally, moving and pressing the optic chiasm, invading the sphenoid sinus and pressing the third cerebral ventricle (Figure 1A and 1B). A chest X‑ray revealed enlargement of the right pulmonary hilum. An abdominal ultrasound performed before hospitalization did not reveal any significant abnormalities. Panhypopituitarism caused by the invasive pituitary mass was diagnosed. Oral hydrocortisone and levothyroxine replacement therapy was administered. Serum and urine osmolality as well as 24‑hour urine volume were not changed markedly. In view of the rapid vision loss, visual field restriction, and optic chiasm compression, the patient was referred for an urgent neurosurgery intervention. The optic chiasm decompression was performed, but this did not improve the patient’s vision. Histopathological evaluation of the pituitary mass revealed small cell carcinoma on immunopositive staining for thyroid transcription factor 1, synaptophysin, neuron‑specific enolase, chromogranin A, and Ki‑67 more than 75% (Figure 1C-1G). Electron microscopy revealed ultrastructural features of small cell carcinoma with small neuroendocrine granules (Figure 1H). An abdominal ultrasound revealed liver metastases, and a definitive diagnosis of small cell lung carcinoma with pituitary and liver metastases was established after bronchofiberoscopy. Palliative chemotherapy was introduced, but the patient died due to neoplasm progression.
Diagnosis and management of the patient with pituitary metastasis are always challenging. Symptomatic metastatic pituitary tumors, although rare, occur in the course of the disseminated neoplasm. The presence of an invasive pituitary mass should prompt a search for malignant proliferative process.
- He W, Chen F, Dalm B, et al. Metastatic involvement of the pituitary gland: a systematic review with pooled individual patient data analysis. Pituitary. 2015; 18: 159‑168. | Crossref
- Komninos J, Vlassopoulou V, Protopapa D, et al. Tumors metastatic to the pituitary gland: case report and literature review. J Clin Endocrinol Metab. 2004; 89: 574‑580. | Crossref
- Marsh JC, Garg S, Wendt JA, et al. Intracranial metastatic disease rarely involves the pituitary: retrospective analysis of 935 metastases in 155 patients and review of the literature. Pituitary. 2010; 13: 260‑265. | Crossref
- Prodam F, Pagano L, Belcastro S, et al. Pituitary metastases from follicular thyroid carcinoma. Thyroid. 2010; 20: 823‑830. | Crossref
- Riemenschneider MJ, Beseoglu K, Hanggi D, et al. Prostate adenocarcinoma metastasis in the pituitary gland. Arch Neurol. 2009; 66: 1036‑1037. | Crossref
ARTICLE INFORMATION