Ovarian fibrothecoma in a young pregnant woman with lupus nephritis undergoing hemodialysis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Ovarian fibrothecoma in a young pregnant woman with lupus nephritis undergoing hemodialysis
Fibrothecoma is a rare tumor that is benign in the majority of cases. It is the most common tumor in the sex cord‑stromal group and represents 1% to 4.7% of the ovarian tumors.1 In more than 90% of cases, it is unilateral and affects postmenopausal women.2 On histopathology, it has fusiform connective tissue and theca‑like cells present in various proportions. Although this tumor is typically asymptomatic and is an accidental finding on imaging, Meigs syndrome may occur. Surgical management remains the best treatment option with a favorable prognosis.3,4
A 26‑year‑old woman was admitted to the hospital during her 28th week of pregnancy due to a mass of uncertain nature on abdominal ultrasound. She had chronic kidney disease stage G5 caused by lupus nephritis in the form of systemic lupus erythematosus–associated tubulointerstitial injury diagnosed at the age of 13 years, proven by a biopsy 3 years later. She was receiving long‑term hemodialysis therapy by arteriovenous fistula for 2 years, had polyclonal gammopathy, and a history of miscarriage at the age of 20 years.
The patient received oral steroid therapy, followed by methylprednisolone and cyclophosphamide pulses because of only partial remission and then progression of chronic kidney disease. Mycophenolate mofetil was started after kidney biopsy. The immunosuppressive therapy was discontinued during pregnancy and dialyses were performed every day.
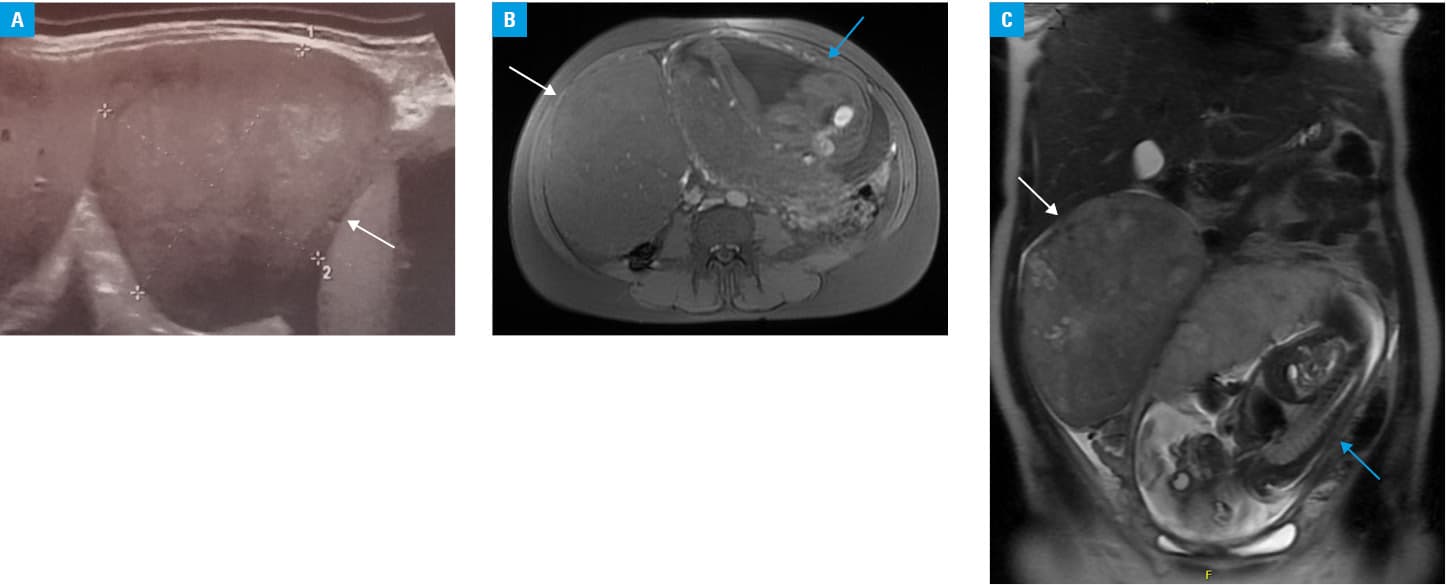
On admission to the hospital, abdominal ultrasonography (Figure 1A) showed a solid mass with smooth margins and moderate vascularity measuring 10 × 9 cm, located in the right mesogastric region. The right ovary was not visualized. Magnetic resonance imaging scan (Figure 1B and 1C) revealed a pathologic mass, measuring 13 × 15 × 17 cm, attached superiorly to the lower segments of the liver and gallbladder, medially to the pregnant uterus, descending below the upper edge of the right ilium, and bordering right uterine appendages, modeling and displacing the bladder. Heterogeneity on T2‑weighted image, intermediate signal intensity on T1‑weighted image, and no restriction in diffusion suggested that the tumor was benign; however, morphology of the lesion suggested dysgerminoma.
Due to preterm labor and imminent fetal asphyxia, an urgent caesarean delivery was performed with simultaneous adnexectomy. The child was born alive. The postoperative period was complicated by Clostridium difficile infection and respiratory insufficiency treated with mechanical ventilation. The symptoms gradually subsided.
Histopathologic examination of the excised mass that was attached to the ovary revealed a solid tumor with central necrotic areas. Neoplasmatic cells were arranged in strands and groups with eosinophilic cytoplasm separated by fusiform cells and connective tissue fibers forming bundles. There were neither mitotic figures nor features of angioinvasion. Neoplastic cells were found close to the ovary border but did not cross the external surface of the gonad. The image indicated fibrothecoma.
In the reported case, ovarian fibrothecoma developed atypically in a premenopausal woman, coexisted with pregnancy, and the tumor growth was very rapid and extensive, which occurs infrequently. In spite of better specificity and accuracy of magnetic resonance imaging in differential diagnosis of pelvic masses, the image was ambiguous.5 Due to pregnancy, unclear nature of the detected tumor, and multiple comorbidities, selection of a proper management was difficult. The association of fibrothecoma with an immune disease, such as systemic lupus erythematosus, and its immunosuppressive therapy should have been considered in this case.
- Slimani O, Ben Temim R, Ajroudi M, et al. Contribution of ultrasound in the study of ovarian fibrothecomas: a series of 47 cases. Tunis Med. 2017; 95: 29‑36.
- Krishnan D, Kumar K, Thomas AA. Unilateral ovarian fibrothecoma with menorrhagia. Malaysian J Pathol. 2014; 36: 55‑58.
- Jung EJ, Eom HM, Byun JM, et al. Different features of the histopathological subtypes of ovarian tumors in pre- and postmenopausal women. Menopause. 2017; 24: 1028‑1032. | Crossref
- Okuda K, Noguchi S, Narumoto O, et al. A case of Meigs’ syndrome with preceding pericardial effusion in advance of pleural effusion. BMC Pulm Med. 2016; 16: 71. | Crossref
- Shinagare AB, Meylaerts LJ, Laury AR, Mortele KJ. MRI features of ovarian fibroma and fibrothecoma with histopathologic correlation. Am J Roentgenol. 2012; 198: 296‑303. | Crossref
ARTICLE INFORMATION