Interleukin-17A contributes to atrial fibrillation recurrence and left atrial reservoir function after catheter ablation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Interleukin-17A contributes to atrial fibrillation recurrence and left atrial reservoir function after catheter ablation
Introduction
Atrial fibrillation (AF) has been linked to an increased long‑term risk of stroke, heart failure, and all‑cause mortality.1 Recently, several studies have been conducted regarding the role of inflammation in the development of AF.2,3 Interleukin 17A (IL‑17A), a pleiotropic proinflammatory cytokine, has been implicated in the development of numerous inflammatory reactions.4,5Some reports have suggested that the expression of IL‑17A is increased in patients with paroxysmal AF.6 However, its role in AF recurrence remains unknown.
Therefore, we aimed to identify predictors of arrhythmia recurrence in patients undergoing catheter ablation (CA) according to the serum levels of IL‑17A. In addition, the changes in IL‑17A levels in patients with AF were assessed for appropriate selection of adjunctive strategies and prognostication of patients undergoing CA.
Patients and methods
Study population
A total of 126 consecutive patients who underwent first‑time CA for paroxysmal AF were prospectively enrolled between March 2015 and March 2016. All patients who had a preserved left ventricular ejection fraction (>55%) were included in the present study. Written informed consent was obtained from each participant, and this study was approved by Ethics Committee of the Affiliated Hospital of Jiangsu University. Exclusion criteria were age <18 years, malignant disease, valvular heart disease or a history of cardiac surgery, hypothyroidism, myocardial infarction, absence of clinical follow‑up, and poor echocardiography images.
Follow‑up
The first 3 months after CA were considered as a blanking period. The presence of an irregular pulse or AF on rhythm monitoring indicated AF recurrence after the blanking period. Patients with no symptomatic AF recurrence or irregular pulse and those requiring no antiarrhythmic agent after the blanking period were assigned into the “no‑recurrence group.” Patients with AF recurrence were assigned to the “AF‑recurrence group.”
Blood samples were taken from patients on the morning of CA (at 6:00 AM), the next day after CA, 3 months, 6 months, 12 months after CA, and following symptom recurrence. Serum levels of IL‑17A, N‑terminal fragment of the prohormone brain natriuretic peptide (NT‑proBNP), matrix metallopeptidase 9 (MMP‑9), procollagen type I, and procollagen type III were measured using a commercial biotin–avidin based sandwich enzyme‑linked immunosorbent assay (eBiosciences, San Diego, California, United States).
Two‑dimensional speckle‑tracking echocardiography
Left atrial (LA) volumes were measured using the Simpson method. The minimum and maximum LA volumes were measured, and the LA emptying fraction (LAEF) was calculated using the following formula: LAEF = (LA volume max – LA volume min) / LA volumemax × 100%. For LAEF measurements, the intraobserver and interobserver variability was 7.2% and 8.4%, respectively.
Electrophysiological study and catheter ablation procedure
Pulmonary vein (PV) isolation was performed in all patients using a previously established method.7 Ablation was guided by a Lasso catheter positioned at the ostium of the PV. Power and temperature settings were set up to 50W, targeting a temperature of 50˚ to 55˚ with a nonirrigated tip catheter. After wide area circumferential ablation, complete disconnection of the PV was the endpoint of the circumferential PV isolation, leading to electrical isolation of all the PVs.
Statistical analyses
Data are shown as means (SD) or as medians with an interquartile range (IQR). Continuous variables were compared with an independent sample t test or analysis of variance as appropriate. The receiver operating characteristic curves were analyzed. Pearson or Spearman correlation tests were used to assess bivariate correlations. A logistic regression analysis was used to explore the role of IL‑17A as an independent predictor of AF recurrence, after controlling for baseline clinical characteristics and echocardiographic parameters. All the analyses were performed using the SPSS software (v. 11.5, SPSS, Chicago, Illinois, United States). A P value of less than 0.05 was considered significant.
Results
Patient characteristics
Patients were divided into 2 groups, with and without clinical AF recurrence. There were 71 patients (56%) who showed sinus rhythm at the last follow‑up and demonstrated clinical success, while 55 patients (44%) experienced recurrence.
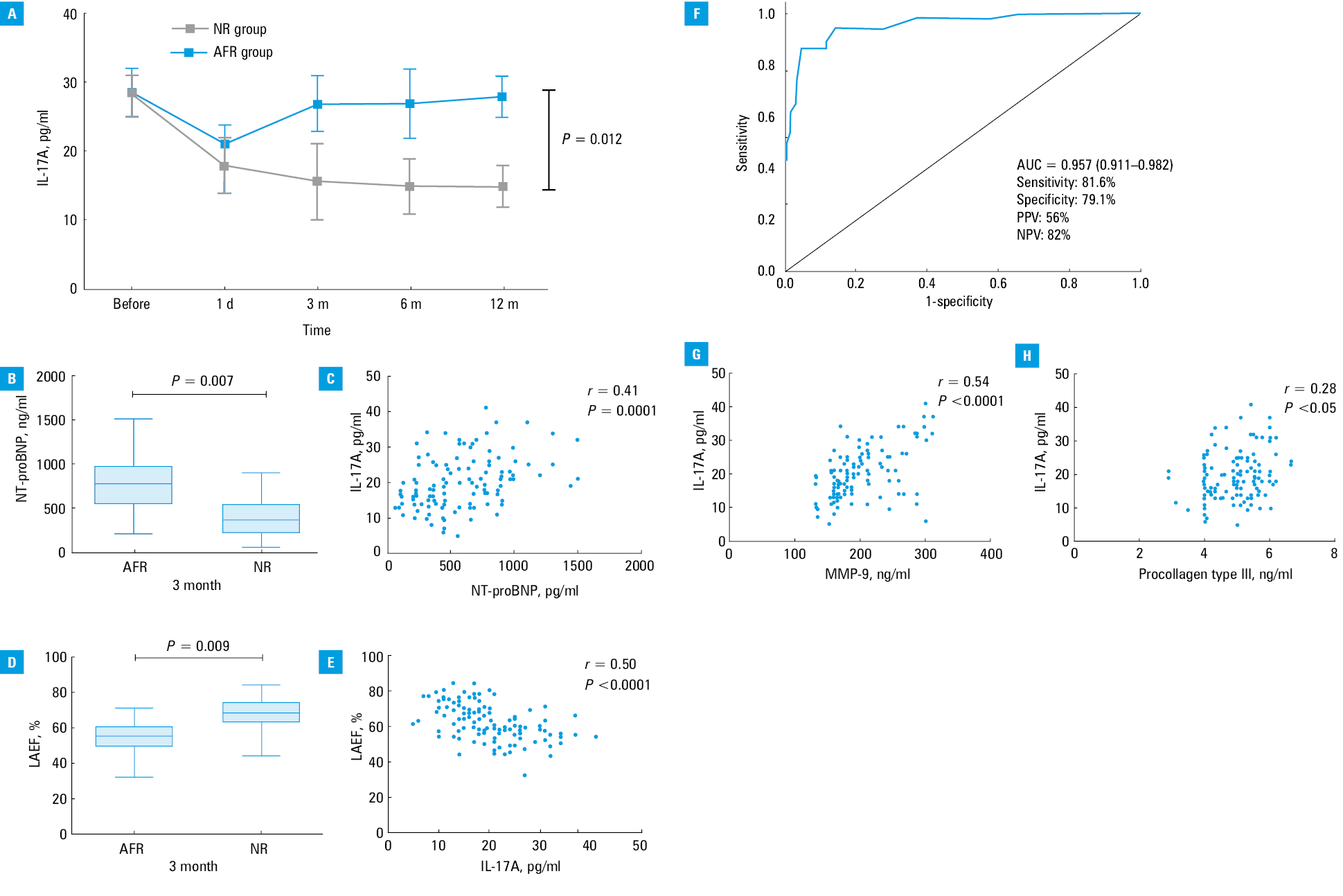
Before CA, there was no significant difference in IL‑17A levels between the AF‑recurrence and no‑recurrence groups. The median follow‑up was 13.1 months (IQR, 4.6–21.4 months). Changes in IL‑17A levels after CA during the 12‑month follow‑up are shown in Figure 1A. On the first day after CA, IL‑17A levels decreased both in the AF‑recurrence and no‑recurrence groups. At 3, 6, and 12 months after CA, the expression of IL‑17A was markedly increased in the AF‑recurrence group. Between 3 and 12 months, the IL‑17A expression remained almost stable. Therefore, we selected the 3‑month follow‑up as the time point for calculating the predictors of AF recurrence. Differences in IL‑17A levels between the AF‑recurrence and no‑recurrence groups are shown in Supplementary material, Table S1. The levels of NT‑proBNP and LAEF at 3‑month follow‑up are presented in Figure 1B and 1C. At 3 months, the LAEF was significantly lower in the AF‑recurrence group, and the NT‑proBNP level was markedly higher in the no‑recurrence group.
Predictors of atrial fibrillation recurrence
We observed a significant correlation between the levels of IL‑17A and NT‑proBNP (r = 0.41, P <0.0001, n = 126; Figure 1D). Moreover, IL‑17A levels correlated with LAEF (r = –0.50, P <0.0001, n = 126; Figure 1E). The receiver operating characteristic curves showed that IL‑17A could be used as a predictor of AF recurrence. The area under the curve was 0.957 (95% CI, 0.911–0.982; P <0.0001; Figure 1F). In the logistic regression analysis, an increase in IL‑17A levels was an independent predictor of AF recurrence (odds ratio, 1.13; 95% CI, 1.04–1.44; P <0.05).
Correlation between fibrosis parameters and serum interleukin 17A levels
To assess whether serum IL‑17A levels were associated with fibrosis parameters, we analyzed the correlations between circulating procollagen type I, procollagen type III, MMP‑9, and IL‑17A. At 3 months, serum IL‑17A levels were positively correlated with the levels of MMP‑9 (r = 0.54, P <0.0001) and procollagen type III (r = 0.28, P <0.05) (Figure 1G and 1H). No correlation was detected between the levels of IL‑17A and procollagen type I (r = 0.12, P = 0.17). Differences in LAEF and the levels of NT‑proBNP, MMP‑9, procollagen type I, and procollagen type III between the AF‑recurrence and no‑recurrence groups at 3‑month follow‑up are shown in Supplementary material, Table S2.
Discussion
In the present study, we demonstrated that serum IL‑17A levels are associated with AF recurrence. Moreover, our main finding is that high expression of IL‑17A at 3 months is an independent predictor of a high risk of AF recurrence after CA.
The most important mechanisms underlying the AF recurrence are inflammatory lesions that occur in the atrium within the first few months following CA.8 While investigating the proinflammatory effects of IL‑17A, we found that its serum expression in the AF‑recurrence group was reduced at day 1 following CA, while it was elevated at 3 months, which is consistent with a trend of increased incidence of AF recurrence.
During ventricular systole, the LA serves as a reservoir to store blood when the aortic valves are closed. The function of this reservoir can be influenced by atrial relaxation and stiffness,9-11 indicating that despite similar atrial dimensions, patients with AF recurrence may have a more pronounced arrythmia substrate, as evidenced by reduced LAEF. In the present study, the IL‑17A level was significantly correlated with LAEF, suggesting that IL‑17A levels could reflect early signs of LV diastolic dysfunction and LA function in patients who undergo first‑time CA for paroxysmal AF. Atrial fibrosis and chamber stiffness may result in the reduction of LAEF, leading to AF recurrence. Therefore, IL‑17A may contribute to AF recurrence by promoting inflammation and cardiac fibrosis.
NT‑proBNP is a powerful prognostic marker of cardiovascular outcomes and mortality, and its expression reflects the structural and functional changes in the heart of patients with AF. Higher serum IL‑17A levels were observed in patients with AF recurrence, which was correlated with higher serum NT‑proBNP levels, suggesting that the IL‑17A level reflects the structural and functional changes in the heart as a result of LV diastolic dysfunction and LA function. Paroxysmal AF contributes to the depression of LA function, which activates IL‑17A signaling. Atrial fibrosis is strongly correlated with AF recurrence. When atrial fibrosis does not occur, normal LA function and IL‑17A levels are restored after CA.
Degradation and accumulation of extracellular matrix play a critical role during LV remodeling.12 In our current study, we showed that the IL‑17A level was strongly correlated with extracellular matrix protein levels in patients with AF recurrence, indicating that IL‑17A may be involved in promoting cardiac fibrosis and LV remodeling.
The transient episodes of recurrent arrhythmia within the 3 months after CA were not considered as AF recurrence because of atrial irritability immediately after CA; therefore, our follow‑up lasted more than 3 months. In summary, our comprehensive and rigorous study indicated that IL‑17A levels measured at 3‑month follow‑up could be used as a predictor of AF recurrence after CA.
A limitation of our study is that there was no long‑term electrocardiographic monitoring to detect subclinical AF. Other limitations include a single‑center design and a small sample size. Therefore, further multicenter research is needed.
In conclusion, the IL‑17A level reflects the structural and functional changes in the heart as a result of LV diastolic dysfunction and LA function, and contributes to AF recurrence by promoting inflammation and cardiac fibrosis. High IL‑17A expression at 3‑month follow‑up is an independent predictor of a high risk of AF recurrence after CA.
- Fuster V, Ryden LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2011; 57: e101‑e198. | Crossref
- Enriquez A, Santangeli P, Zado ES, et al. Postoperative atrial tachycardias after mitral valve surgery: mechanisms and outcomes of catheter ablation. Heart rhythm. 2017;14: 520‑526. | Crossref
- Iwakura Y, Ishigame H, Saijo S, et al. Functional specialization of interleukin‑17 family members. Immunity. 2011; 34: 149‑162. | Crossref
- Song X, Qian Y. IL‑17 family cytokines mediated signaling in the pathogenesis of inflammatory diseases. Cell signal. 2013; 25: 2335‑2347. | Crossref
- Wu N, Xu B, Liu Y, et al. Elevated plasma levels of Th17‑related cytokines are associated with increased risk of atrial fibrillation. Sci Rep. 2016; 6: 26543. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION