Omental splenosis after liver transplantation for hepatocellular carcinoma mimicking metastasis on fluoro-18-deoxyglucose positron emission tomography with computed tomography



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Omental splenosis after liver transplantation for hepatocellular carcinoma mimicking metastasis on fluoro-18-deoxyglucose positron emission tomography with computed tomography
Splenosis is an acquired condition defined as seeding and autotransplantation of splenic tissue following splenic trauma or splenectomy. It should be distinguished from the accessory spleen.1 Although it is usually benign, correct identification is essential because misdiagnosis can have a significant impact on patient management.
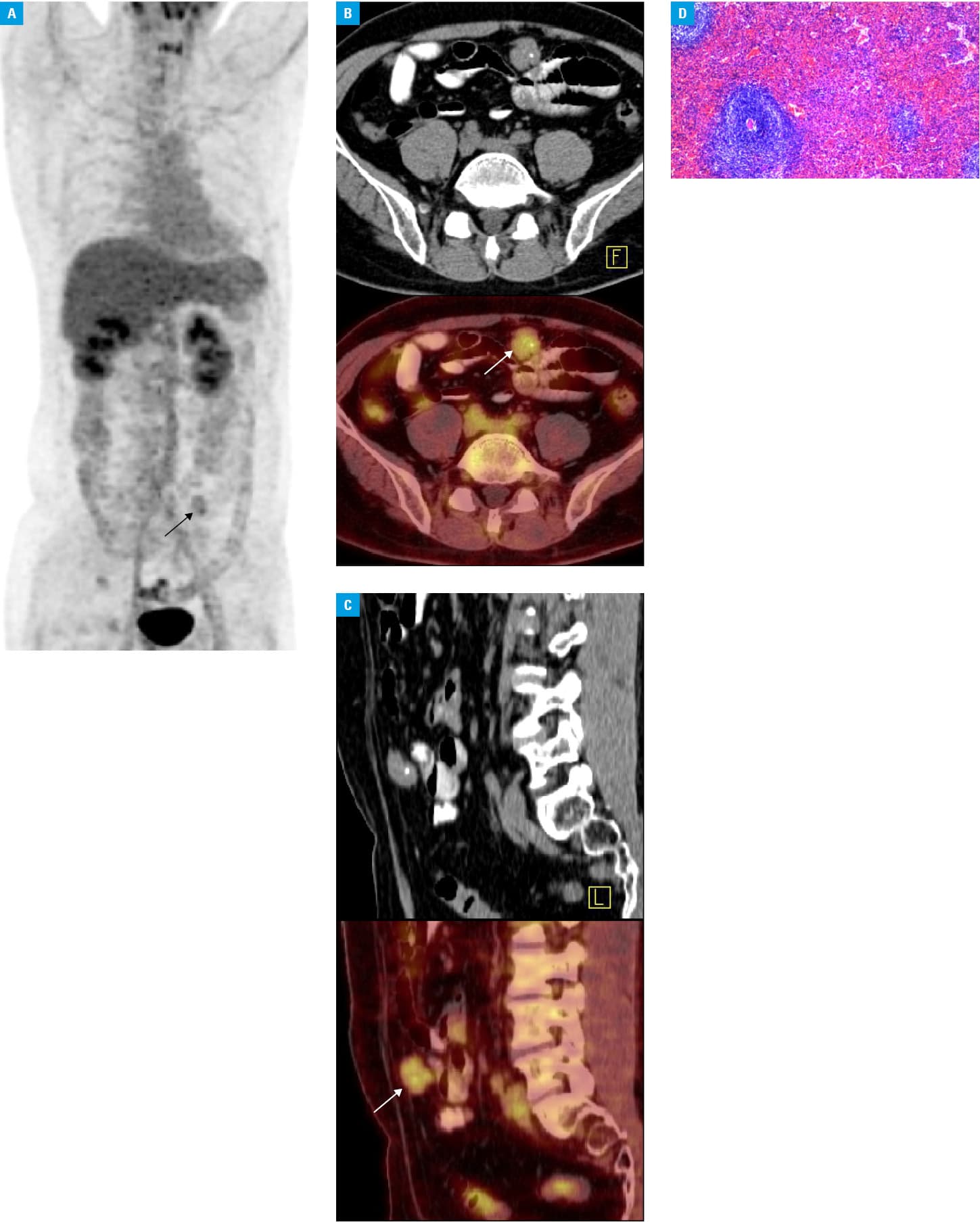
An asymptomatic 48‑year‑old man after transplantation was admitted for routine checkup. He had a history of hepatocellular carcinoma associated with hepatitis B cirrhosis and hypersplenism, which had been treated by liver transplantation and splenectomy 6 years earlier. The level of α-fetoprotein was slightly elevated (32 μg/l). Abdominal ultrasonography revealed a 2.3‑cm, well‑circumscribed intra‑abdominal hypoechoic mass. Considering the possibility of a metastatic lesion, a fluoro‑18‑deoxyglucose (18F‑FDG) positron emission tomography (PET) coregistered with a computed tomography (CT) scan was performed. It demonstrated a lesion in the lower abdomen (Figure 1A), located in the greater omentum. It showed central calcification on CT and the corresponding fused images (Figures 1B and 1C), with a moderate 18F‑FDG uptake in relation to the lesion (maximum standardized uptake value, 3.88). No other abnormal distribution of 18F‑FDG was shown. Accordingly, the biopsy of the mass was performed, and histologic examination revealed marked lymphoid‑like tissue background and many sinusoidal structures, consistent with spleen structure (Figure 1D). Based on these findings, omental splenosis was diagnosed.
On conventional imaging, such as ultrasonography and CT, identifying splenosis remains challenging due to its nonspecific imaging characteristics.1,2 At present, splenic imaging with heat‑denatured red blood cells labeled with technetium‑99m can allow a definitive diagnosis and avoid surgical resection, and has been accepted as a noninvasive technique for detecting splenic tissue.3 However, to our knowledge, reports on splenosis mimicking metastasis on 18F‑FDG PET‑CT are scarce. In our patient, iatrogenic rupture of the spleen might have contributed to omental splenosis. This case highlights that splenosis can mimic metastasis on 18F‑FDG PET/CT in oncologic patients who had undergone splenectomy. Thus, to avoid an unnecessary surgery, splenosis should be considered in a differential diagnosis of newly discovered solitary or multiple lesions located anywhere in the peritoneal and thoracic cavities.
- Tsitouridis I, Michaelides M, Sotiriadis C, Arvaniti M. CT and MRI of intraperitoneal splenosis. Diagn Interv Radiol. 2010; 16: 145‑149.
- Grande M, Lapecorella M, Ianora AA, et al. Intrahepatic and widely distributed intraabdominal splenosis: multidetector CT, US and scintigraphic findings. Intern Emerg Med. 2008; 3: 265‑267. | Crossref
- Vásquez Tineo SI, García lonso MP, Mendoza Paulini A, et al. Non‑invasive diagnosis of posttraumatic thoracic splenosis. Rev Esp Med Nucl. 2011; 30: 311‑313. | Crossref
ARTICLE INFORMATION