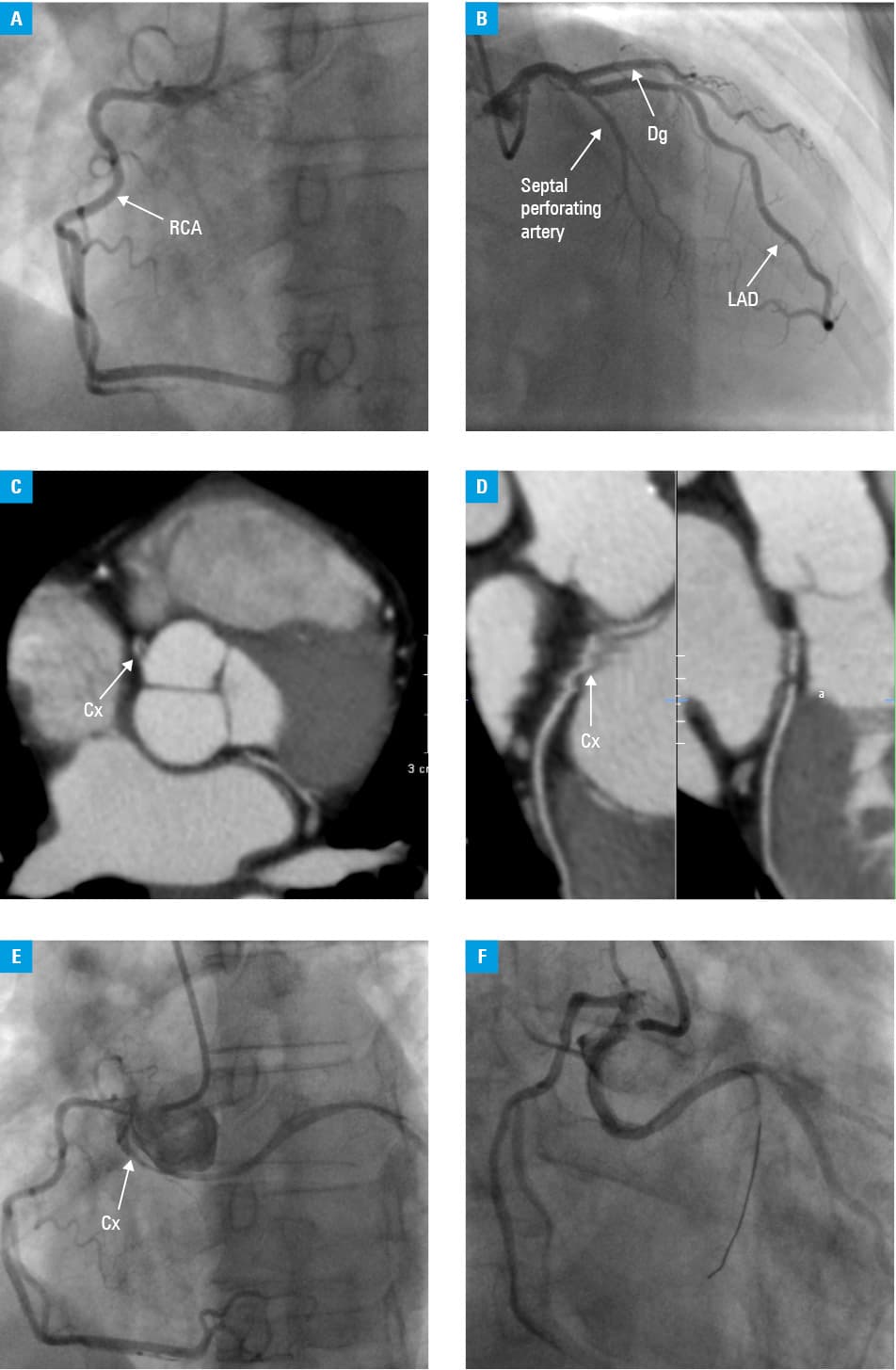
A 48-years-old patient with non–ST-elevation myocardial infarction caused by a narrowing in the anomalous circumflex artery



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A 48-years-old patient with non–ST-elevation myocardial infarction caused by a narrowing in the anomalous circumflex artery
Coronary artery anomalies are rare findings with an incidence of 0.3% to 1.5%.1 The circumflex branch of the left coronary artery (Cx) arising from the right coronary artery or from the right Valsalva sinus is the most common type of such malformations.1 They are considered to be asymptomatic, although cases of exertional pain, myocardial infarction, or even sudden cardiac death have been reported.2,3 We present a case of a patient with non–ST‑elevated myocardial infarction caused by critical stenosis of the ectopic Cx.
A 48‑years‑old man was admitted to the emergency department with acute onset of typical angina. He did not have any risk factors for atherosclerosis except for being a heavy smoker for 30 years. After the confirmation of non–ST‑elevated myocardial infarction, the patient was redirected to the catheterization laboratory. On admission, the patient had no chest pain, his blood pressure was 139/76 mm Hg, and heart and lung auscultation was normal. Electrocardiography did not reveal any abnormalities. Lateral and inferior wall hypokinesis of the left ventricle with preserved ejection fraction were observed on the echocardiographic examination. Coronary artery angiography revealed no significant atherosclerotic stenoses in the right or left coronary arteries (Figure 1A and 1B). Lack of Cx led to the suspicion of coronary anomaly. Therefore, computed tomography of the coronary arteries (angio‑CT) was performed and exposed Cx originating in the right sinus of Valsalva with a possible narrowing within (Figure 1Cand 1d). The second coronary angiography confirmed ectopic Cx with significant stenosis, and percutaneous coronary angioplasty with drug eluting stent implantation was performed (Figure 1E and 1f). After a few days of recovery, the patient was discharged home.
The current follow‑up is 4 months from the time of percutaneous coronary intervention and none of the coronary artery disease symptoms were reported. An electrocardiographic exercise treadmill test was negative with 14.2 metabolic equivalents achieved.
Although anomalies of the coronary arteries are usually accidentally found on coronary angiography or autopsy, they may be the cause of serious medical conditions. Also in cases of anomalous Cx, which is considered a benign malformation, life‑threatening cardiac events may occur due to the compression of the ectopic artery by the great vessels. Another possible pathophysiological mechanism is accelerated atherosclerosis in the anomalous artery as in the presented patient.4
Ectopic coronary arteries may cause numerous technical problems even for greatly experienced operators. They may depart not only from different parts of the aortic bulb and ascending aorta but also from the pulmonary trunk.5 In these situations, additional imaging techniques such as angio‑CT or magnetic resonance scans are valuable diagnostic methods. When abnormal artery origination is suspected, we should strive for its visualization at all costs because it may completely change the diagnosis, and may save lives by using proper treatment.
- Alexander RW, Griffith GC. Anomalies of the coronary arteries and their clinical significance. Circulation. 1956; 14: 800‑805. | Crossref
- Taylor AJ, Byers JP, Cheitlin MD, Virmani R. Anomalous right or left coronary artery from the contralateral coronary sinus: “high‑risk” abnormalities in the initial coronary artery course and heterogeneus clinical outcomes. Am Heart J. 1997; 133: 428‑435. | Crossref
- Piovesana P, Corrado D, Verlato R, et al. Morbidity associated with anomalous origin of the left circumflex coronary artery from the right aortic sinus. Am J Cardiol. 1989; 63: 762‑763. | Crossref
- Samarendra P, Kumari S, Hafeez M, et al. Anomalous circumflex coronary artery: benign or predisposed to selective atherosclerosis. Angiology. 2001; 52: 521‑526. | Crossref
- Cowles RA, Berdon WE. Bland‑White‑Garland syndrome of anomalous left coronary artery arising from the pulmonary artery (ALCAPA): A historical review. Pediatric Radiology. 2007; 37: 890‑895. | Crossref
ARTICLE INFORMATION