Usefulness of trabecular bone score in a misdiagnosed case of osteoporosis: clinical image of a woman with multiple fractures



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Usefulness of trabecular bone score in a misdiagnosed case of osteoporosis: clinical image of a woman with multiple fractures
Trabecular bone score (TBS) is a new diagnostic tool that improves identification of new patients who are at risk of fractures due to the deteriorated bone microarchitecture. Currently, bone mineral density (BMD) assessment is the gold standard for osteoporosis diagnosis. However, a number of fractures occur in patients with osteopenia.1 In addition, TBS has been considered a BMD‑independent risk factor for fractures.
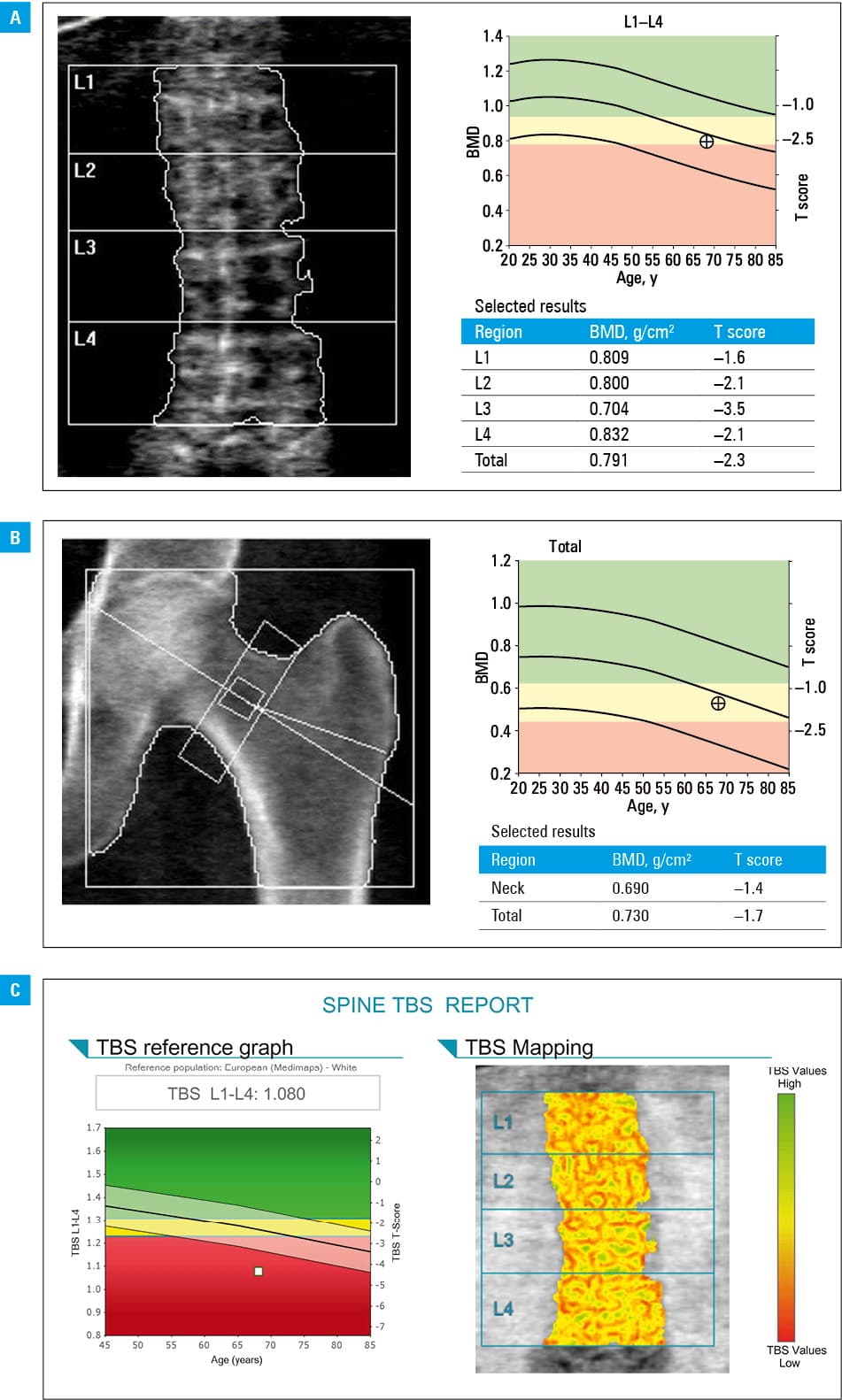
We report the case of a 68‑year‑old postmenopausal woman who experienced pelvic, thoracic, and lumbar spine pain without any previous injury. Computed tomography revealed advanced bone loss, compression fractures of the L1, L2, L5 vertebral bodies, hemangioma in the L3 vertebral body, fractures of the Th10, Th11 vertebral bodies, the lower right pubic bone branch, and lateral surface of the sacral bone. Basic laboratory tests, calcium, phosphorus, vitamin D, thyroid stimulating hormone, parathyroid hormone concentrations, serum protein electrophoresis, calcium and phosphorus 24‑hour excretion remained within normal ranges. Additionally, the patient complained of heartburn, and gastroscopy revealed gastroesophageal reflux. Dual X‑ray absorptiometry (DXA) of the spine was performed (Figure 1A). Unfortunately, L1, L2, L3 vertebral bodies could not be evaluated because of compression fractures in L1 and L2 and hemangioma in L3. DXA of the proximal femur revealed total hip T score of –1.7 corresponding to osteopenia (Figure 1B). As the physicians were convinced that she has severe osteoporosis, the distal one‑third of radius DXA of the nondominant forearm was performed, which indicated osteopenia with a T score of –1.9 (Supplementary material, Figure S1). Additionally, TBS of the spine was evaluated and revealed markedly deteriorated bone microarchitecture (Figure 1C). The patient received denosumab due to contraindications for oral bisphosphonates.
The evaluation of TBS is possible using a software compatible with densitometers. It helps assess the microarchitecture of trabecular bone on the spine DXA images as it shows the bone texture inhomogeneity (“holes” and “fills”). Studies have shown an incremental improvement in fracture prediction when TBS is used with the Fracture Risk Assessment Tool (FRAX).2 The official position of the International Society of Clinical Densitometry (ISCD) is that TBS values are associated with risk of vertebral, proximal femur, and other major osteoporotic fractures in postmenopausal women and in men over the age of 50 years. Trabecular bone score can be used with the FRAX calculator to predict fractures. However, TBS should not be used alone to decide on a treatment in clinical practice, because it is not currently included in the guidelines.2,3 Falsely high results due to osteoarthritis are not shown on TBS, which is its great advantage. Furthermore, TBS may play a role in the evaluation of fracture risk in secondary osteoporosis (ie, primary hyperparathyroidism, glucocorticoid‑induced osteoporosis, etc).2,4,5
In our case, TBS L1–L4 numerical value was 1.080, which points to markedly deteriorated bone microarchitecture. Values above 1.35 are considered correct, between 1.2 to 1.35, intermediate, and below 1.2, incorrect, indicating osteoporosis.4
Our case shows that TBS identifies patients who are presently underdiagnosed, because they do not meet the BMD criteria of osteoporosis.
- Cranney A, Jamal S, Tsang J, et al. Low bone mineral density and fracture burden in postmenopausal women. CMAJ. 2007; 177: 575‑580. | Crossref
- Kanis JA, Cooper C, Rizzoli R, Reginster JY. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019; 30: 3‑44. | Crossref
- Martineau P, Leslie WD. The utility and limitations of using trabecular bone score with FRAX. Curr Opin Rheumatol. 2018; 30: 412‑419. | Crossref
- Tay YD, Cusano NE, Rubin MR, et al. Trabecular bone score in obese and nonobese subjects with primary hyperparathyroidism before and after parathyroidectomy. J Clin Endocrinol Metab. 2018; 103: 1512‑1521. | Crossref
- Florez H, Hernández‑Rodríguez J, Muxi A, et al. Trabecular bone score improves fracture risk assessment in glucocorticoid‑induced osteoporosis. Rheumatology (Oxford). 2019 Oct 19. . | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION