A large amount of pericardial fluid: determining consecutive steps in the diagnosis and treatment of pulmonary arterial hypertension



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A large amount of pericardial fluid: determining consecutive steps in the diagnosis and treatment of pulmonary arterial hypertension
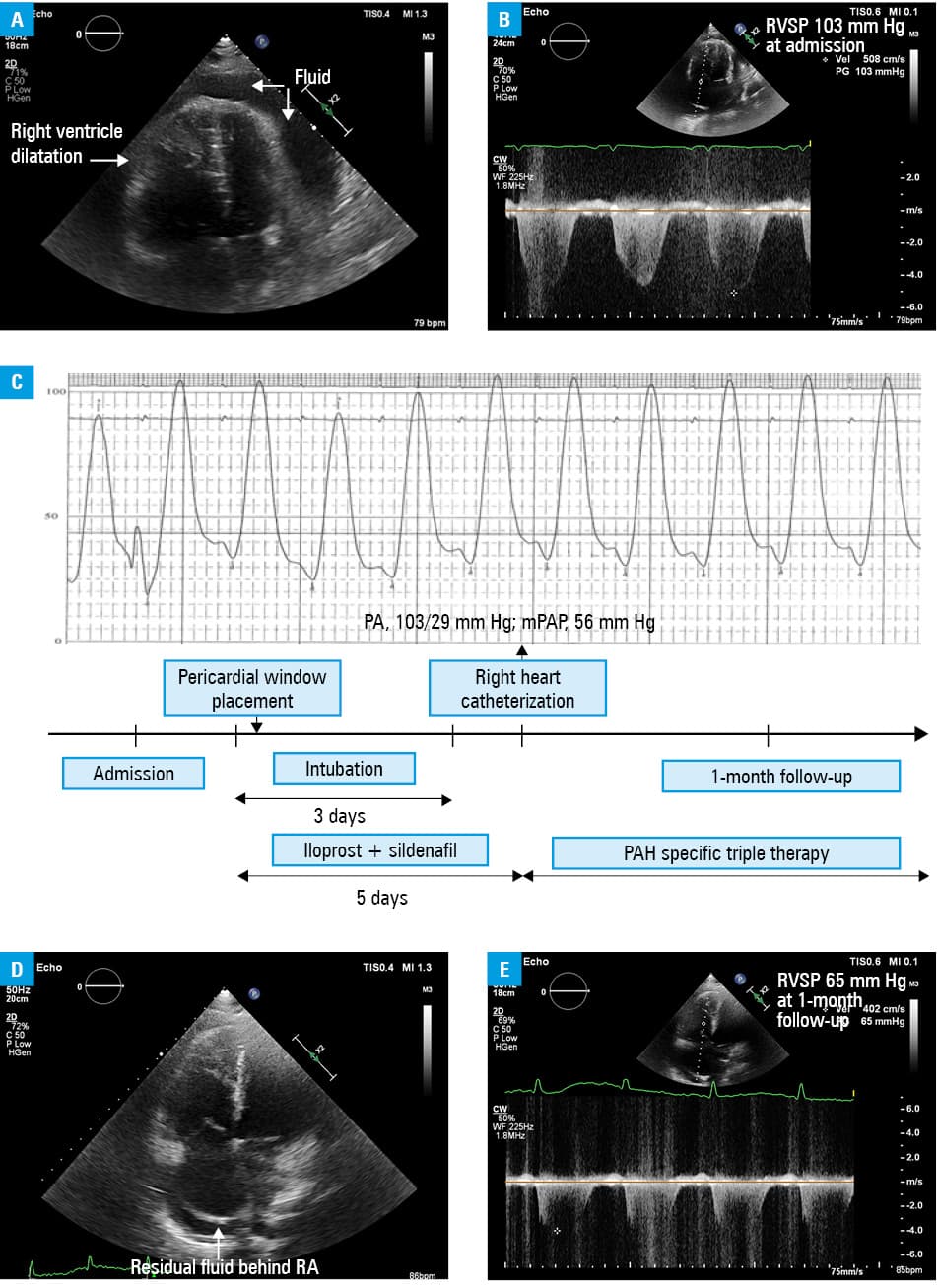
A 41‑year‑old woman with systemic scleroderma was admitted to a reference pulmonary hypertension center1 due to severe fatigue and dyspnea, the New York Heart Association (NYHA) class IV, that started about 6 months before admission. Transthoracic echocardiography demonstrated a significant amount of fluid (30 mm) around the right atrium and ventricle. Additionally, dilatation of the pulmonary artery, the right atrium (area 25 cm2), and the right ventricle (52 mm) with extremely high estimated right ventricle systolic pressure (103 mm Hg) were revealed (Figure 1Aand 1B). Laboratory tests identified an elevated N‑terminal pro‑B‑type natriuretic peptide level (4579 pg/ml). Based on these data, pulmonary arterial hypertension (PAH) in the course of connective tissue disease was hypothesized. We assumed that the pericardial fluid did not result in tamponade because of elevated right heart pressures. However, this seemed as a contraindication to PAH‑specific treatment due to high risk of tamponade after a sudden pressure reduction.2 Percutaneous pericardiocentesis was unavailable due to extreme obesity (body mass index, 41 kg/m2) and limited amount of fluid around the apex of the heart (Supplementary material, Figure S1). The patient was referred to the cardiac surgery department, where surgical drainage was performed by a pericardial window placement. The cardiosurgical intervention provided drainage of 1000 ml of serous fluid and hemodynamic stability was achieved. Meanwhile, iloprost and sildenafil were administered during the periprocedural period and mechanical ventilation, which reduced pulmonary artery pressure and allowed extubation on the third day after the procedure. In terms of the diagnostic workup, right heart catheterization was performed, which confirmed severe PAH (mean pulmonary artery pressure, 56 mm Hg; reference range, 10–20 mm Hg; pulmonary vascular resistance, 9.64 Wood units [mm Hg/l min-1]; reference range, 0.25–2.5 Wood units; negative vasoreactivity test with iloprost) (Figure 1C). The patient received specific medical therapy including sildenafil, bosentan, and treprostinil. As a result, patient’s symptoms reduced to class II according to the World Health Organization Pulmonary Hypertension Functional Classification which was confirmed by transthoracic echocardiography at 1‑month follow‑up. (Figure 1Dand 1E).
Pulmonary arterial hypertension is a multicausal disease related to increased mortality. The prevalence of pericardial effusion among patients with PAH was estimated at 26%.3 A greater amount of fluid may occur in patients with connective tissue disease. However, this rarely exceeds 10 to 20 mm.4 The presence of pericardial effusion has been identified as a risk factor for cardiac death.5 Patients with a small pericardial effusion had similar survival to those without effusion, but patients with PAH who had a moderate to large pericardial effusion had significantly decreased survival.5 In our patient, we observed a large pericardial effusion with the characteristics of a transudative effusion. The etiology of effusion was complex and superposed on PAH with systemic scleroderma. We were aware that medical therapy, including endothelin receptor antagonists, phosphodiesterase type 5 inhibitors, and prostacyclin derivatives, might have improved the prognosis of the patient. However, crucial decisions were made to ensure safety and effectiveness, and were related to an appropriate order of the diagnostic workup and treatment. First, cardiosurgical intervention along with a life‑saving PAH treatment and then right heart catheterization and PAH‑specific multiagent therapy. Gradually administered drugs helped to avoid a sudden decrease in mean pulmonary artery pressure, which could have caused hemodynamic instability.
- Kopeć G, Kurzyna M, Mroczek E, et al. Characterization of patients with pulmonary arterial hypertension: data from the Polish Registry of Pulmonary Hypertension (BNP‑PL). J Clin Med. 2020; 9: 173. | Crossref
- Khan MU, Khouzam RN. Protective effect of pulmonary hypertension against right‑sided tamponade in pericardial effusion. South Med J. 2015; 108: 46‑48. | Crossref
- Fenstad ER, Le RJ, Sinak LJ, et al. Pericardial effusions in pulmonary arterial hypertension. Chest. 2013; 144: 1530‑1538. | Crossref
- Campo A, Mathai SC, Le Pavec J, et al. Hemodynamic predictors of survival in scleroderma‑related pulmonary arterial hypertension. Am J Respir Crit Care Med. 2010; 182: 252‑260 | Crossref
- Shimony A, Fox BD, Langleben D, et al. Incidence and significance of pericardial effusion in patients with pulmonary arterial hypertension. Can J Cardiol. 2013; 29: 678‑682. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION