Interferon beta-1a for patients with moderate to severe acute respiratory distress syndrome: a systematic review and meta-analysis of randomized trials
Key words: acute respiratory distress syndrome, interferon beta-1a, interferon therapy, mortality, systematic review



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Interferon beta-1a for patients with moderate to severe acute respiratory distress syndrome: a systematic review and meta-analysis of randomized trials
Introduction: Acute respiratory distress syndrome (ARDS) is a life‑threatening disease characterized by respiratory failure with rapidly progressing inflammation. Currently, no effective pharmacological treatment for ARDS is available.
Objectives: We conducted this systematic review and meta‑analysis to examine the use of interferon beta‑1a in patients with ARDS.
Methods: Data sources included the following databases: MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials. We retained trials from 1996 to February 25, 2020 that comparatively examined the use of interferon beta‑1a in patients with ARDS. Two reviewers identified eligible studies, independently extracted study data, and assessed the risk of bias. The authors evaluated the certainty of evidence using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.
Results: We included 2 trials (n = 392 patients). No significant differences in 28‑day hospital mortality (risk ratio [RR], 0.59; 95% CI, 0.13–2.67; P = 0.49; very low certainty) and the number of ventilator‑free days (mean difference, 4.85 days; 95% CI, –3.25 to 12.93; P = 0.24, very low certainty) were observed in patients treated with interferon beta‑1a compared with those not receiving this drug. Interferon beta‑1a also had no significant impact on the risk of adverse events (RR, 0.98%; 95% CI, 0.94–1.03; P =0.47; low certainty).
Conclusions: The use of interferon beta‑1a does not appear to improve mortality or reduce the number of ventilator‑free days and adverse events in patients with ARDS. This review is based on 2 small studies reporting a limited number of events, which raises questions regarding the true effects of interferon beta‑1a. The analysis of 1 study revealed increased mortality with the concomitant use of corticosteroids and interferon beta‑1a, suggesting a need for careful consideration of this drug–drug interaction.
What's new?
Acute respiratory distress syndrome (ARDS) is a life‑threatening inflammatory pulmonary process, characterized by rapid progression and the need for respiratory support. There is no specific pharmacological therapy for ARDS. We conducted a systematic review and meta‑analysis on the use of interferon beta‑1a in ARDS by searching 3 electronic databases. The eligible studies were critically appraised and assessed with respect to quality of evidence. Our review of 2 randomized controlled trials suggests that interferon beta‑1a does not reduce mortality or duration of mechanical ventilation. The subgroup analysis of one of the studies stratified by corticosteroid use showed increased mortality associated with the use of corticosteroids and interferon beta‑1a. This suggests that careful consideration of drug–drug interactions is required when multiple pharmacological therapies are administered.
Introduction
Acute lung injury can lead to an inflammatory pulmonary process, which rapidly progresses to acute respiratory distress syndrome (ARDS), a highly fatal respiratory disease characterized by diffuse alveolar damage.1-3Mortality in ARDS can be as high as 40%, with incidence rates reaching 78 cases per 100000 individuals.3,4 If triggered by both infectious and noninfectious etiologies, ARDS has an early, or exudative, phase manifested by increased pulmonary capillary permeability, leading to alveolar fluid accumulation and worsened oxygenation.5 Mortality rises with disease severity and patient’s age, and outcomes range from complete resolution to substantial chronic lung damage.3 Interferon beta‑1a has been shown to reduce pulmonary capillary permeability and posited as a therapeutic candidate for ARDS.6 Currently, the treatment of ARDS is based principally on supportive care, management of the underlying disease, and ventilator support.7
Preliminary evidence from a small, open‑label, phase 1/2 study revealed some benefit of reducing 28‑day mortality in patients with ARDS treated with interferon beta‑1a compared with those treatment‑naive.6 Acute respiratory distress syndrome is associated with severe morbidity and mortality. That is why we sought to clarify evidence on the safety and efficacy of a potentially beneficial treatment. We conducted this systematic review and meta‑analysis to determine the efficacy of interferon beta‑1a in patients with ARDS.
Methods
Data sources and search methods
A protocol with predetermined eligibility criteria and methods was developed for this review. Given the global emergency situation and the present delay in the International Prospective Register of Systematic Reviews, we proceeded with this rapid review without formal registration.
The following databases were searched: 1) MEDLINE/PubMed (1996 to February 25, 2020), applying a search filter for randomized controlled trials (RCTs) with no limits; 2) EMBASE (1996 to February 25, 2020), filtering for RCTs; and 3) the Cochrane Central Register of Controlled Trials (to February 25, 2020), with no limits (for an exemplary search in the MEDLINE and EMBASE databases, see Supplementary material, Appendix S1).
Study selection
Eligible studies were comparative, parallel‑group RCTs that randomized patients with ARDS, of any cause, to the interferon beta‑1a therapy versus placebo or standard treatment or no treatment. We sought studies reporting on at least 1 of the following outcomes: all‑cause mortality, duration of mechanical ventilation, length of hospital stay, ventilator‑free days (defined as the number of days alive free from mechanical ventilation), or adverse effects and complications associated with the use of interferon beta‑1a. If a study reported outcomes at more than 1 time point, we abstracted data closest to the longest follow‑up. Two reviewers independently screened titles and abstracts in duplicate, obtained full texts of articles that either reviewer considered potentially eligible, and determined the final review eligibility of the full texts.
Data abstraction and quality assessment
Two reviewers, independently and in duplicate, extracted relevant data (study design, study demographics such as author, year, location and center status, patient demographics such as age, sex, sample size, intervention [the timing of interferon beta‑1a initiation and dosing regimens], comparator, and outcomes that included all‑cause mortality, duration of mechanical ventilation, number of ventilator‑free days, and adverse events), and assessed the risk of bias (performed critical appraisal) using the Cochrane risk of bias tool8 for RCTs. During the TA and FT phases, screening was performed in duplicate and independently by pairs of screeners. Disagreement was settled by consensus or with adjudication of a third party if necessary. We also assessed 2 additional domains that were considered potential factors for a high risk of bias (stopping early for benefit and baseline imbalance). We adopted the following response options regarding the risk of bias: “yes,” “probably yes,” “probably no,” and “no,” aiming to remove the often provided “unclear” responses, which limit a clear interpretation of the risk of bias.9
To assess the overall risk of bias, we judged whether the key domains (randomization, allocation concealment, blinding of patients and healthcare providers, data loss, and stopping early for benefit) were optimally reported. If any of the domains were not demonstrated as optimally executed, then the study was assigned a high risk of bias (Supplementary material, Table S1).
Data synthesis and analysis
We used random‑effects modeling for all analyses with the Mantel–Haenszel risk ratio (RR) for dichotomous outcomes and mean difference (MD) for continuous variables.10 We hypothesized that a greater severity of ARDS and a higher risk of bias would be associated with a larger treatment effect. We were aware of the fact that the analysis would be limited by the comprehensiveness of study reporting. If data were reported as median and interquartile range, we converted these to mean (SD).11
We conducted subgroup analyses by the severity of ARDS, as well as dose and early versus late administration of interferon beta‑1a, if the reported data allowed to do so. We also performed sensitivity analyses, excluding studies at high risk of bias, to assess the robustness of estimates. Studies stopped early for benefit were flagged.12 The aim of the sensitivity analysis was to separate studies at high risk of bias and examine their effect on the pooled estimate.
We conducted the meta‑analyses using the Review Manager software, version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). We assessed heterogeneity by visual inspection of forest plots, a statistical test for heterogeneity, and the I2 statistic (with results >50% considered as significant heterogeneity).8,12
We reported 95% CI with the presented estimates of effect. To estimate the absolute effects of the intervention, we sought large RCTs providing the best estimates of these outcomes. The control event rate was used to estimate the baseline risk in computing the absolute effects. To determine the absolute effect, we multiplied the baseline risk by the relative effect (and 95% CIs). We considered assumptions based on the worst‑case scenario: the best‑case assumption modeling, if data loss (attrition) was reported, was deemed to have impact on the effect.13
GRADE methods
We adopted the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach to rate the certainty of evidence for each outcome and the entire body of evidence.14 We sought patient outcomes that we judged to be critical and relevant to patients (and clinicians) in informed decision making.
Definition of acute respiratory distress syndrome
If data could support the subgroup analysis by the severity of ARDS (degree of hypoxemia), we defined ARDS in terms of the Berlin definition developed in 2011 (based on an initiative of the European Society of Intensive Care Medicine endorsed by the American Thoracic Society and the Society of Critical Care Medicine).15 It includes 3 mutually exclusive categories of ARDS, characterized by the degree of hypoxemia: 1) mild (200 <PaO2/FiO2 ≤300), 2) moderate (100 < PaO2/FiO2 ≤200), and 3) severe (PaO2/FiO2 ≤100), and 4 ancillary variables for severe ARDS: radiographic severity, respiratory system compliance (≤40 ml/cm H2O), positive end‑expiratory pressure (≥10 cm H2O), and corrected expired volume per minute (≥10 l/min).
Results
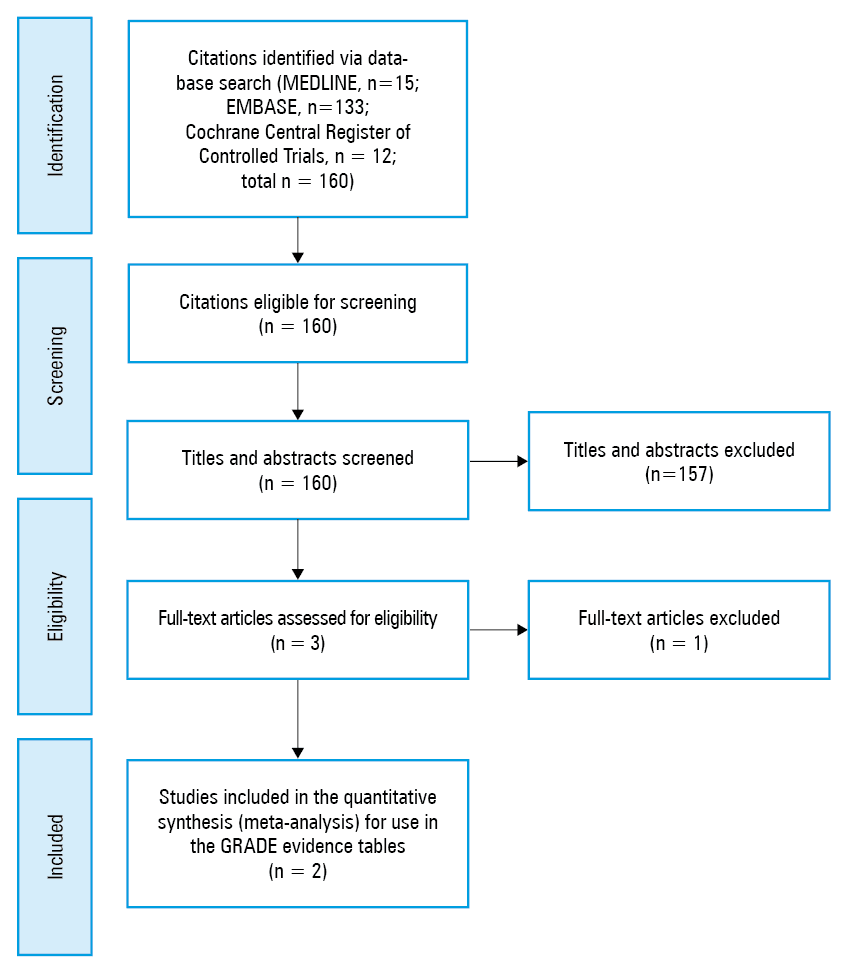
We found 2 clinical trials that met our inclusion criteria.6,16 This was based on identifying initially a total of 160 citations: 15 in the MEDLINE database, 133 in the EMBASE database, and 12 in the Cochrane Central Register of Controlled Trials. Full texts of 3 studies were screened and 2 trials were retained for the final systematic review (for the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses17 flow diagram, see Figure 1).
Study characteristics
The detailed study characteristics are presented in Table 1. The 2 primary studies included were multicenter and funded by both public and private resources. Sample sizes ranged from 96 to 296 (used for analysis) hospitalized patients, mostly men (>60% in both studies), typically over 50 years of age. Patients received interferon beta‑1a versus placebo and interferon beta‑1a versus no intervention.6,16Follow‑up ranged from 28 to 180 days.6,16 The main causes of ARDS reported in both trials were pneumonia, sepsis, and aspiration, in that order.
Study | Sample sizea | Male sex, %; age | Inclusion criteria | Follow‑up | Treatment intervention arm, dose vs treatment control arm, dose | Degree of hypoxemia or lung injury | Reported cause of ARDS | Notable comorbidities |
a Data are presented as total number of study patients; number of patients in the intervention arm; number of patients in the control arm.
b Severe ARDS was defined as PaO2/FiO2 <100 (mm Hg) (<13.3 [kPa]) with PEEP >5 cm H2O, and moderate ARDS as PaO2/FiO2 >100 (mm Hg) (>13.3 [kPa]) and <200 (mm Hg) (<26.6 [kPa]) with PEEP >5 cm H2O
Abbreviations: ARDS, acute respiratory distress syndrome; FP‑1201, interferon beta‑1a; FiO2, fraction of inspired oxygen; HIV, human immunodeficiency virus; PaO2, partial oxygen pressure; PEEP, positive end‑expiratory pressure | ||||||||
Bellingan et al,6 United Kingdom, multicenter | 96; 37; 59 | 60.4%; treatment arm, median (IQR), 52 (40–67) y; control arm, median (IQR), 61 (47–71) y | Age ≥18 y, ARDS with bilateral pulmonary infiltrates, PaO2/FiO2 ratio ≤40 (kPa), no evidence of elevated left atrial pressure, treated with assisted ventilation | 28 days to 6 months, for mortality | A daily intravenous dose of FP‑1201 for 6 days
Control group: no drug intervention; patients who met the inclusion criteria (but were not recruited, most commonly because they were diagnosed during 1 of the safety windows of nonrecruitment [41 patients], although, in a smaller number of cases, it was related to consent issues [eg, decision time exceeding the 48‑hour window for inclusion; 18 patients]) | PaO2/FiO2 (kPa), median (IQR): 19 (14–24) in the treatment group vs 19 (13–25) in the control group | Pneumonia, sepsis, aspiration, surgery, pancreatitis, HIV, other | Unclear |
Ranieri et al,16 international, multicenter | 301 randomized (5% of randomized patients did not receive intervention as randomized); 144 in the primary analysis; 152 in the primary analysis | 65.2%; treatment arm, mean (SD), 58 (17) y; placebo arm, mean (SD), 58 (14) y | Age >18 y, intubated and mechanically ventilated, with moderate or severe ARDS according to the Berlin definition
The radiological and PaO2/FiO2 criteria had to be met within a 24‑hour period, and administration of the first dose of the study drug had to occur within 48 hrs after the diagnosis of ARDS. | 28 days for primary endpoints; otherwise, to 180 days | Patients received either intravenous 10-μg interferon beta‑1a or placebo once daily for 6 days. The placebo consisted of the same excipients as the intervention drug, except interferon beta‑1a. Administration of the first dose had to take place within 48 hrs after the diagnosis of ARDS. | Treatment group: 28 patients with severe ARDS, 116 with moderate ARDS
Placebo group: 35 patients with severe ARDS, 117 with moderate ARDSb
Tidal volume, median (IQR): 417 (372–470) ml in the treatment group vs 423 (380–472) ml in the placebo group
Inspiratory pressure, mean (SD): 29.9 (6.8) cm H2O in the treatment group vs 31.1 (7.6) in the placebo group | Pneumonia, sepsis, aspiration, acute pancreatitis, trauma/burns, multiple transfusions, other | Patients received support at randomization, including corticosteroids, vasopressor support, neuromuscular blocking agents, renal replacement therapy, prone positioning
Note: interpreting the results, it should be considered that corticosteroids may have an impact on the biological effect of interferon beta‑1a. |
Risk of bias assessment
One6 of the 2 trials (50%) was judged to be at high risk of bias (Table 2). The loss to follow‑up was rare and less than 5% if occurred. Therefore, worst- and best‑case plausible modeling assumptions about the outcomes of patients lost to follow‑up were not required. We also decided to develop no funnel plots or statistical tests for publication bias due to the limited interpretability, which is observed when the number of studies is less than 10, as in this review.
Study | Randomization and allocation concealment | Blinding of patients | Blinding of healthcare providers | Blinding of data collectors | Blinding of adjudicators | Blinding of data analysts | Selective outcome reporting | Attrition | Baseline imbalance | Stopping for benefit | Other bias issues | Funding | Overall risk of bias |
Bellingan et al6 | Probably no (very unclear reporting on randomization, particularly regarding the control group) | No | No | Probably no | Probably no | Probably no | No | No | No | No | No | Public and private | High |
Ranieri et al16 | Yes | Yes | Probably yes | Probably yes | Probably yes | Probably yes | No | No | No | No | Yes; in the interpretation of results, corticosteroids may have had an impact on the biological effect of interferon beta‑1a. | Public and private | Low‑to‑moderate |
Outcomes
28‑day in‑hospital mortality
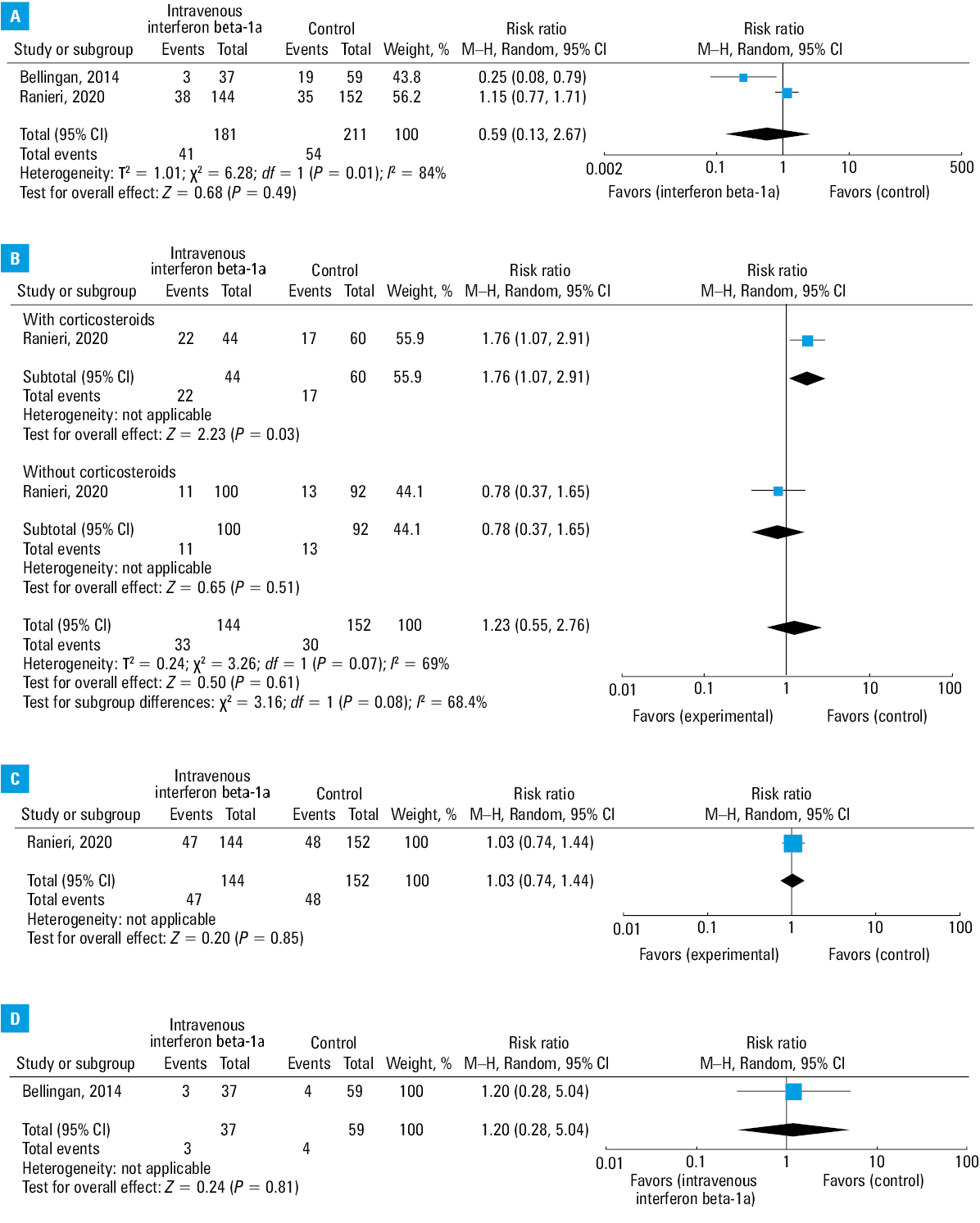
Two trials6,16(including 392 patients) reported on 28‑day in‑hospital mortality and revealed a nonsignificant difference, whereby 41 of 181 patients (22.6%) died in the group treated with interferon beta‑1a compared with 54 of 211 (25.6%) in the control group (RR, 0.59; 95% CI, 0.13–2.67; P = 0.49; I2 = 84%; very low certainty of evidence) (Figure 2A). The very small number of studies did not allow for subgroup analyses based on the severity of ARDS. Absolute effects were 105 fewer deaths per 1000 affected individuals (from 223 fewer to 427 more) (for the GRADE evidence profile, see Table 3).
Certainty assessment | Patients, n (%) | Effect | Certainty | Importance | ||||||||
Studies, n | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Interferon beta‑1a | Control/placebo | Relative (95% CI) | Absolute (95% CI) | ||
a Very unclear reporting on randomization, particularly regarding the control group. In the study by Ranieri et al,16 corticosteroids may have had an impact on the biological effect of interferon beta‑1a, as patients were also given corticosteroids.
b A significant P = 0.01 as per the Cochran’s Q χ2 test, I2 =84%
c A small number of events and studies, 95% CI crossing benefits and harms
d Optimal information amount not provided
e Optimal information amount provided only in 1 study; very wide 95% CI (benefits and harms)
f Regarding the interpretation of results, corticosteroids may have had an impact on the biological effect of interferon beta‑1a.
g Heterogeneity: P <0.0001, I2 =98%
h Optimal information amount provided; very wide 95% CI (benefits and harms); a small number of studies
i Unclear reporting on randomization, particularly regarding the control group
Abbreviations: MD, mean difference; RR, risk ratio | ||||||||||||
28‑day in‑hospital mortality (follow‑up, 28 days) | ||||||||||||
2 | Randomized trial | Seriousa | Seriousb | Not serious | Seriousc | None | 41/181 (22.7) | 54/211 (25.6) | RR, 0.59 (0.13–2.67) | 105 fewer deaths per 1000 individuals (range, from 223 fewer to 427 more) | Very low | Critical |
Serious adverse events (follow‑up, 28 days) | ||||||||||||
1 | Randomized trial | Seriousf | Not serious | Not serious | Seriouse | None | 138/144 (95.8) | 148/152 (97.4) | RR, 0.98 (0.94–1.03) | 19 fewer adverse events per 1000 individuals (range, from 58 fewer to 29 more) | Low | Critical |
Ventilator‑free days to hospitalization day 28 (follow‑up, 28 days) | ||||||||||||
2 | Randomized trial | Seriousa | Seriousg | Not serious | Serioush | None | 181 | 211 | – | MD, 4.85 days more (range, 3.24 fewer to 12.93 more) | Very low | Critical |
90‑day mortality in patients treated with corticosteroids (follow‑up, median, 90 days) | ||||||||||||
1 | Randomized trial | Not serious | Not serious | Not serious | Seriouse | None | 47/144 (32.6) | 48/152 (31.6) | RR, 1.03 (0.74–1.44) | 9 deaths more per 1000 individuals (from 82 fewer to 139 more) | Moderate | Critical |
180‑day mortality in patients treated with corticosteroids (follow‑up, median, 180 days) | ||||||||||||
1 | Randomized trial | Seriousi | Not serious | Not serious | Seriousd | None | 3/37 (8.1) | 4/59 (6.8) | RR, 1.2 (0.28–5.04) | 14 deaths more per 1000 individuals (from 49 fewer to 274 more) | Low | Critical |
Subgroup analysis: 28‑day in‑hospital mortality stratified by corticosteroid use
Due to the reported posthoc analysis on the use of corticosteroids, we present the evidence although we did not intend to conduct an analysis based on nonintervention treatment regimens. One trial16 (including 296 patients) reported on 28‑day in‑hospital mortality stratified by corticosteroid use, and the subgroup test for interactions was nonsignificant with P = 0.08. Of note, although Ranieri et al,16 reporting on 28‑day mortality, noted 38 deaths in the group treated with interferon beta‑1a and 35 in the control group, the number of deaths stratified by corticosteroid use is inconsistent with the primary outcome assessment with the following implied values for 28‑day mortality: 33 deaths (50% of 44, 28.3% of 60) in the corticosteroid‑treated group and 30 (10.6% of 100, 14.8% of 92) in the control group.
There was a significant increase in the mortality risk in the subgroup treated with both corticosteroids and interferon beta‑1a (RR, 1.76; 95% CI, 1.07–2.91; P = 0.03) (Figure 2B).
Absolute effects were 215 more deaths per 1000 affected individuals (from 20 more to 541 more) (for the GRADE evidence profile, see Table 3).
In contrast, no significant differences in mortality were reported in the subgroup treated with interferon beta‑1a and not receiving corticosteroids (RR, 0.78; 95% CI, 0.37–1.65; P = 0.51) (Figure 2B). Absolute effects were 31 fewer deaths per 1000 affected individuals (from 89 fewer to 92 more) (for the GRADE evidence profile, see Table 3).
90‑day in‑hospital mortality
One trial16 (including 296 patients) reported on 90‑day in‑hospital mortality and showed a nonsignificant difference, whereby 47 of 144 patients (32.6%) died in the group treated with interferon beta‑1a compared with 48 of 152 (31.6%) in the control group (RR, 1.03; 95% CI 0.74–1.44; P = 0.85; very low certainty) (Figure 2C). Absolute effects were 9 more deaths per 1000 affected individuals (from 82 fewer to 139 more) (for the GRADE evidence profile, see Table 3).
180‑day in‑hospital mortality
Data on 180‑day in‑hospital mortality were also available. One trial16(including 296 patients) reported on 180‑day in‑hospital mortality and demonstrated a nonsignificant difference, whereby 3 of 37 patients (8.1%) died in the group treated with interferon beta‑1a compared with 4 of 59 (6.8%) in the control group (RR, 1.2; 95% CI, 0.28–5.04; P = 0.81; very low certainty) (Figure 2D). Absolute effects were 14 fewer deaths per 1000 affected individuals (from 49 fewer to 247 more) (for the GRADE evidence profile, see Table 3).
Ventilator‑free days up to hospitalization day 28
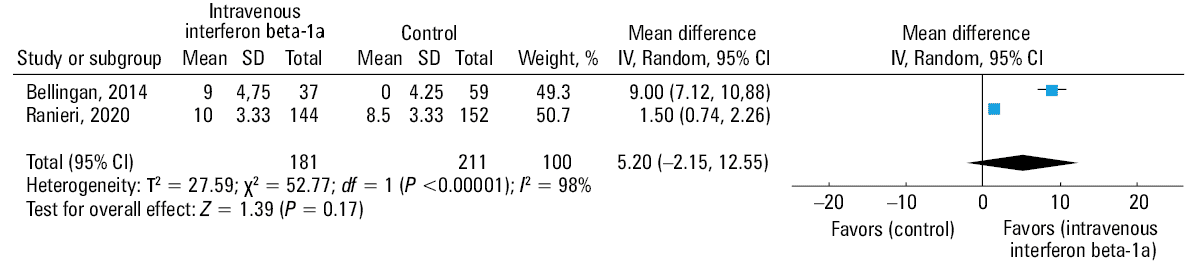
Both trials6,16(including a total of 392 patients) examined the number of ventilator‑free days up to hospitalization day 28 and showed a nonsignificant increase in the mean number of ventilator‑free days in patients receiving interferon beta‑1a (MD, 4.85 days; 95% CI, –3.24 to 12.93; P = 0.24; I2 = 98%; very low certainty) (Figure 3). The absolute difference was 4.85 more ventilator‑free days (from 3.24 days fewer to 6.94 days more) (for the GRADE evidence profile, see Table 3).
Serious adverse events
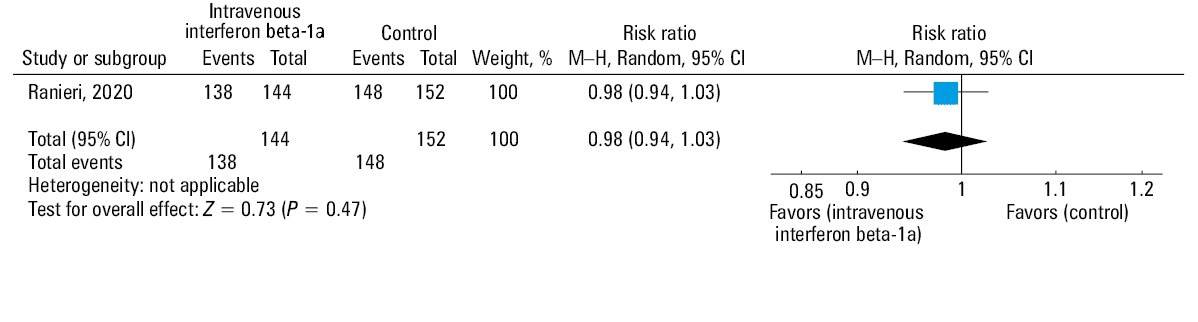
One trial16(including 296 patients) reported on serious adverse events and revealed a nonsignificant impact on serious adverse events, whereby 138 of 144 patients (95.8%) had an adverse event in the group treated with interferon beta‑1a compared with 148 of 152 (97.3%) in the control group (RR, 0.98; 95% CI, 0.94–1.03; P = 0.47; very low certainty) (Figure 4). The absolute effects were 19 fewer adverse events per 1000 affected individuals (from 58 fewer to 29 more) (for the GRADE evidence profile, see Table 3).
Discussion
Our systematic review and meta‑analysis examined the effect of the interferon beta‑1a treatment in patients with ARDS. Since there were 2 small studies examining this issue, we pooled the studies to increase power and detect a difference in the effects. The review showed no significant differences in mortality (at 28, 90, or 180 days) or the number of ventilator‑free days. Similarly, there were no differences in serious adverse effects. For 28‑day mortality, no significant subgroup interaction was noted in patients receiving corticosteroids versus those treatment‑naive, but a significant increase in mortality was observed in patients receiving corticosteroids and interferon beta‑1a. Although the subgroup interactions were nonsignificant with P = 0.08, it may be relevant to relay the possible subgroup interactions given the small number of patients and more common use of corticosteroids in ARDS. However, due to suboptimal outcome reporting noted in the primary outcome analysis, with the posthoc mortality counts not matching the totals, we urge caution in the interpretation of the results stratified by corticosteroid use. Overall, the outcomes were downgraded to very low certainty of evidence using the GRADE approach, and the certainty of evidence was principally downgraded due to an increased risk of bias, a low number of studies, small sample sizes, imprecision, and heterogeneity.
We had very low confidence in the absolute risk decrease estimate of 10.5% fewer deaths (regarding 28‑day mortality) per 100 adult patients with ARDS treated with interferon beta‑1a (Figure 2A and Table 3). Furthermore, the studies included in the review reported evidence of a very low certainty that the number of ventilator‑free days in this population was increased by approximately 4.8 days on average (Figure 3and Table 3). In addition, we found low‑certainty evidence on the absolute risk decrease estimate of 1.5% of fewer adverse events per 100 patients treated with interferon beta‑1a (Figure 4 and Table 3). The randomization was not clearly reported, which impacted our risk of bias assessment.
Our study had several strengths. First, we developed explicit eligibility criteria based on the characteristics of patients with ARDS and conducted a comprehensive search using 3 electronic databases. Moreover, we assessed the eligibility of uncovered studies and the risk of bias in duplicate and independently to address the relevant outcomes. We also conducted 1 plausible subgroup test regarding the corticosteroid use.
Although infectious conditions such as pneumonia and sepsis can precipitate ARDS, noninfectious etiologies such as acute pancreatitis and drug reactions are also possible.1,18 Acute respiratory distress syndrome leads to a rapidly progressive inflammatory pulmonary process in the acute exudative phase and, subsequently, to diffuse alveolar damage, damage to the endothelial hyaline membranes, and fibrin deposition, which is likely regulated by inflammatory mediators.18 As interferon beta‑1a increases CD73 and extracellular adenosine levels, it is postulated to reduce capillary permeability, a mechanistic target for ARDS.19,20
In a promising, initial, prospective, open‑label study, interferon beta‑1a appeared to reduce mortality.16 These positive results prompted a large, prospective, randomized, comparative study on the effectiveness of interferon beta‑1a compared with placebo, which showed no significant differences in the primary mortality outcomes.6
Interestingly, the combination of corticosteroids and interferon beta‑1a was reported to increase mortality in patients with ARDS, and interferon beta‑1a administered without corticosteroids was associated with no significant differences in mortality. However, a recently published, large, prospective RCT on the use of corticosteroids in ARDS suggested an association between decreased mortality and corticosteroid use.21 These results imply a drug–drug interaction between the 2 agents, since both participate in various immunological pathways, which may converge.22 The drug–drug interaction between interferon beta‑1a and corticosteroids may lead to diverging effects. It should be discerned whether this observation negates the putative benefits of each drug in ARDS or results in a significant synergy in immunosuppression, which intensifies infection and causes death.
The emerging evidence from a trial16 on the use of interferon beta‑1a raises numerous questions and does not clarify the evidence landscape for treating patients with ARDS. This may be a result of a small study sample size with a relatively small number of adverse events. Moreover, the recent outbreak of coronavirus disease 2019 (COVID‑19) in Wuhan, China, which has spread across the globe, causing acute lung injury and ARDS, invokes interest in treatment options for ARDS and speculation regarding the possible treatment of patients with severe COVID‑19.23
Corticosteroid use in ARDS appears to reduce mortality and duration of mechanical ventilation, while increasing the number of ventilator‑free days.3 Apart from that, there are other promising treatments for ARDS. Researchers are investigating statins, beta‑agonists, neuromuscular blocking agents, and surfactants.2
This review suggested that interferon beta‑1a is not a treatment candidate for ARDS due to the limited evidence on its effectiveness in ARDS. There is no evidence of benefit related to the use of interferon beta‑1a, and we have very low confidence in our pooled estimates of effect.
Our study also had several limitations. For pragmatic reasons, we could not search the grey literature or conference abstracts, and thus we may have omitted some possibly eligible studies. Furthermore, we noted significant statistical heterogeneity in the pooled estimates of mortality and ventilator‑free days.
Conclusions
The use of interferon beta‑1a appears to cause no significant improvement in mortality nor reduction in the number of ventilator‑free days in patients with ARDS. The clinical heterogeneity of ARDS pathogenesis requires urgent research. Increased mortality associated with the concomitant use of interferon beta‑1a and corticosteroids imply an antagonistic interaction between the 2 agents, since both are involved in various immunological pathways, which may converge. The interplay between interferon beta‑1a and corticosteroids may drive diverging effects that negate the putative benefits of each individual drug in ARDS. Suitably powered and methodologically strong clinical studies on large patient samples with sufficiently long follow‑up are needed in patients with ARDS treated with interferon beta‑1a.
- Force ADT, Ranieri V, Rubenfeld G, et al. Acute respiratory distress syndrome. JAMA. 2012; 307: 2526‑2533. | Crossref
- Lewis SR, Pritchard MW, Thomas CM, Smith AF. Pharmacological agents for adults with acute respiratory distress syndrome. Cochrane Database Syst Rev. 2019; 7: CD004477. | Crossref
- Maca J, Jor O, Holub M, et al. Past and present ARDS mortality rates: a systematic review. Respir Care. 2017; 62: 113‑122. | Crossref
- Rezoagli E, Fumagalli R, Bellani G. Definition and epidemiology of acute respiratory distress syndrome. Ann Transl Med. 2017; 5: 282. | Crossref
- Matthay MA, Zemans RL, Zimmerman GA, et al. Acute respiratory distress syndrome. Nat Rev Dis Primers. 2019; 5: 1‑22. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION