The necessity of prevention and treatment in the population of adolescents based on a comprehensive health assessment: the SOPKARD-Junior study



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The necessity of prevention and treatment in the population of adolescents based on a comprehensive health assessment: the SOPKARD-Junior study
Introduction
One of the most important goals of any health policy should be to protect the health of children and adolescents.1 Preventive strategies in the population aged 18 years or younger have 2 basic goals: the detection of diseases at the earliest stages and the search for risk factors of civilization diseases. This is crucial because prevention in a young person makes it possible to reduce the incidence of many diseases throughout their life. The number of studies assessing the prevalence of individual diseases in adolescents is increasing, while epidemiological studies that would assess health of children and adolescents in a holistic way are still missing. Lack of a comprehensive assessment of the state of health with simultaneous search for risk factors of civilization diseases in this population precludes the implementation of holistic screening models and, consequently, adequate preventive measures.
The main objective of the study is to comprehensively assess the health status of adolescents and to identify needs in the area of prevention and therapy. Understanding these needs will allow for the development of an optimal model of screening assessments and basic educational activities for teenagers. Therefore, an additional goal of the study is to propose a panel of screening assessments based on the epidemiological situation of adolescent health.
Patients and methods
The study was carried out from October 2013 to December 2013 and from October 2014 to December 2014 as part of 2 editions of the Program For the Early Detection of Risk Factors for Civilization Diseases SOPKARD‑Junior. All students aged 14 years attending gymnasiums (Polish counterparts of junior high schools) in Sopot, Poland in the given year were invited to participate. Participants were recruited in September 2013 and September 2014, accordingly. The city of Sopot was chosen because of its proximity to the Medical University of Gdańsk and the University Clinical Centre in Gdańsk, Poland and very good cooperation with the local government that has supported this project for many years.
Anthropometric and blood pressure (BP) measurements, echocardiography, orthopedic, psychological‑psychiatric, and dental assessments as well as biochemical blood and urine tests were performed. Orthopedic, echocardiography, psychologic‑psychiatric, and dental assessments were performed by doctors with experience in the specific area. Generally, the assessments in the SOPKARD‑Junior program have been designed to enable the identification of 3 groups of children: group 1 including those with results within the age‑specific norm; group 2 including those with borderline results; group 3 including those with abnormal results or a diagnosis.
A detailed methodology of this study, which is part of the SOPKARD‑Junior program, was described previously.2
Anthropometric assessment included measurements of height and body mass, and calculation of the body mass index (BMI) (calculated as BMI = weight in kg/[height in m]2). Obtained results were compared with centile charts valid for the Polish population.3 Adolescents with normal body weight (>5th to <85th percentile) were included in group 1, those with overweight (≥85th and <95th percentile) and underweight (>3rd and ≤5th percentile), in group 2; while those with obesity (≥95th percentile) or malnutrition (≤3th percentile), in group 3.
Blood pressure was measured 3 times during 1 visit at 2‑minute intervals. The mean of the second and third readings was used in the analysis. The mean systolic and diastolic BP values were compared with the up‑to‑date centile charts for the Polish population.4 The mean BP values below the 90th percentile were assumed to be normal. The mean BP values between the 90th and less than 95th percentile were qualified as high‑normal, and the mean BP values equal to, or greater than 95th percentile were considered elevated. Finally, adolescents whose mean values of both systolic and diastolic pressure were within the normal range were included in group 1. Group 2 included those with high‑normal mean systolic or diastolic BP. Group 3 included those with elevated mean values of systolic or diastolic BP.
Echocardiography was performed with the GE Vivid 95E Cardiac Ultrasound System (standard views in 2‑dimensional‑mode, M‑mode, and color Doppler mode; General Electric Healthcare, Chicago, Illinois, United States) with simultaneous recording of 1 electrocardiography (ECG) lead. The results obtained were compared with weight‑specific norms. Based on the echocardiography, adolescents were classified into 3 groups: group 1 including those without any abnormalities; group 2 including those with abnormalities of low hemodynamic significance, such as patent foramen ovale (PFO), pulmonary insufficiency, tricuspid insufficiency, which may worsen in the future and therefore require periodic cardiac assessments; and group 3 including those with newly diagnosed or pre‑existing heart disease requiring cardiac care (heart defects, cardiomyopathies, aortic insufficiency, mitral insufficiency).
Diagnostic workup of caries as part of dental examination was performed using the visual‑tactile method. The mouth was illuminated by a front electric lamp and the diagnostic kit (World Health Organization periodontal probe and dental mirror) was used for the detection of caries (primary and secondary lesions were diagnosed where the cavity was softer than the tooth tissue, excluding stains and discoloration of noncarries origin and developmental disorders of the enamel), fillings, and teeth removed due to caries.5 Group 1 included adolescents who had never had caries (D + M + F = 0, where D stands for decayed, M stands for missing, and F stands for filled). Group 2 included those without active carious process (D = 0) but with at least 1 filling (F >0) and/or tooth lost due to caries (M >0). Group 3 included those with active caries (D + M + F >0, where D >0; M ≥0; F ≥0). Obtained data were recorded in a dental chart and then analyzed to assess the DMF index and the frequency of caries (group 2 and 3) in students participating in the study.
Blood samples were collected from every patient after 8 to 12 hours of fasting and an overnight rest. First morning urine specimens were delivered the same day in the container received at the initial meeting. The following biochemical tests were performed: C‑reactive protein, electrolytes, thyroid‑stimulating hormone, creatinine, total cholesterol (TC), high‑density lipoprotein cholesterol (HDL‑C), triglycerides (TG), blood glucose, and peripheral blood cell count. Low‑density lipoprotein cholesterol (LDL‑C) level was calculated using the Friedewald formula.6 A urinalysis was performed and potassium, sodium, creatinine, and albumin levels were determined in the morning urine samples. All assays were performed at the Central Clinical Laboratory of the University Clinical Centre in Gdańsk, which is recorded in the Register of the National Chamber of Laboratory Diagnostic (no. 1661).
Each result of a biochemical test was assigned to 1 of the 3 groups: group 1 including results within the age‑specific normal range; group 2 including borderline results (between normal concentration and abnormal concentration); group 3 including abnormal result.
Measured values of TC, TG, LDL‑C, and HDL‑C were used to assess the cardiovascular risk. According to the experts of the National Education Cholesterol Program, the results of children and adolescents are classified into 3 groups: normal acceptable, borderline, and elevated values according to centile charts.7,8 The purpose of the carbohydrate metabolism evaluation was to determine fasting glucose levels. If after the first determination the result did not fit into the reference values (≥100 mg/dl),9 the patient was invited again for additional measurement (second step). Thyroid stimulating hormone (TSH) assays were used to assess thyroid function.10 In order to find the earliest indicators of kidney damage, the urinary albumin‑to‑creatinine ratio (UACR)11,12 was used. Additionally, serum creatinine and general urinalysis were assessed. The reference values that allow classifying the results obtained to particular groups are presented in Table 1.
Variable | Normal (acceptable) levels (group 1) | Threshold (borderline) levels (group 2) | High levels (group 3) | |
Abbreviations: HDL‑C, high‑density lipoprotein cholesterol; NA, not applicable; TC, total cholesterol; TG, triglycerides; TSH, thyroid‑stimulating hormone; UACR, urinary albumin‑to‑creatinine ratio | ||||
TC, mg/dl | <170 | 170–199 | ≥200 | |
TG, mg/dl | <90 | 90–129 | ≥130 | |
HDL‑C, mg/dl | >45 | 35–45 | ≤35 | |
TSH, mU/l | 11–14 years of age | <4.61 | NA | ≥4.61 |
15–18 years of age | <4.33 | NA | ≥4.33 | |
Glucose, mg/dl | 70–99 | NA | ≥100 | |
UACR, mg/g | <30 | NA | ≥30 | |
During orthopedic analysis, static and dynamic body posture assessments were performed with particular emphasis on the foot and ankle. Adolescents who did not show any deviations from the age norm (normal-arched foot posture or stage I pes planovalgus) were qualified to group 1. Group 2 included those with stage II and III pes planovalgus with generalized soft tissue laxity (Marshall test) in whom complete correction was observed in unloaded state and dynamic testing. Group 3 included those with uncorrectable flat foot (including those with incomplete correction), contracture of the gastrocnemius muscle, asymmetric valgus deformity, and other diseases of the musculoskeletal system requiring further diagnosis and treatment.
As part of psychological and psychiatric assessment, the severity of depressive symptoms and the prevalence of depression were evaluated. In the first step, the Beck Depression Inventory was administered to all the examined adolescents. In the second step, students with depressive symptoms were invited to undergo a psychiatric examination. As a result of these assessments, 3 groups of adolescents were distinguished: group 1 including healthy children who showed no depressive symptoms in the screening test; group 2 including those at risk who showed depressive symptoms in the screening test (Beck Depression Inventory score >10 points); and group 3 including those who were diagnosed with clinical depression based on medical psychiatric examination. Adolescents with depressive symptoms who did not report for a clinical evaluation to a child psychiatrist were qualified to group 2.
Data regarding the occurrence of individual health problems were supplemented on the basis of detailed interviews with parents. Parents filled out a questionnaire containing questions about chronic diseases in their child. If the parent said that the child, for example, had diabetes, he or she was automatically qualified to group 3.
The final overall assessment of the health status of each child was performed by analyzing the results using the weighted burden analysis. Group 1 was assigned the weight of 100 points, group 2, 50 points, and group 3, 0 points. The obtained scores were summed up and the arithmetic mean was calculated for each child. Adolescents who participated in at least 5 assessments were included in the analysis. The program has been approved by an independent bioethics committee (assigned numbers, NKEBN/510/2006, NKEBN/510‑350/2007, NKEBN/510‑364/2009, NKBBN/510‑249/2012, NKBBN/510‑403/2014, NKBBN/278/2016).
Statistical analysis
Qualitative data are presented as frequency (percentage). Statistical analysis was performed using the R statistical package, version 3.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
The only condition that had to be met for a teenager to be included in the program was obtaining the written consent of the teenager and his or her legal guardian. After the study, parents received individual information cards with their child’s medical results.
Results
Overall, 337 junior high school students were invited to participate in the SOPKARD‑Junior program implemented in 2013 and 2014, of which parents of 282 students (83.7%; 133 girls and 149 boys) gave their written consent to their child’s participation in the program. The mean age of adolescents was 14 years and 5 months (SD, 0.6; range, 13 years and 4 months to 15 years and 4 months).
The percentages of the adolescents included in groups 1, 2, and 3 are presented in Table 2. The highest percentage of adolescents included in group 3 was observed in dental examinations (49.2%), followed by orthopedic (26.3%), lipid profile (21.2%), and anthropometric assessments (12.3%). Detailed results of orthopedic examination are presented in Supplementary material, Tables S1 and S2.
Examination | Group 1 | Group 2 | Group 3 |
Data are presented as number (percentage).
a Including overweight, 38 (14.2) and underweight, 6 (2.2)
b Including obesity 26 (9.7) and malnutrition 7 (2.6)
c A total of 73 children (out of 79 qualified) attended the second step of psychological and psychiatric examinations
Abbreviations: BMI, body mass index; ECG, electrocardiography; others, see Table 1 | |||
BMI | 191 (71.3) | 44 (16.4)a | 33 (12.3)b |
Blood pressure | 240 (89.5) | 19 (7.1) | 9 (3.4) |
Echocardiography and ECG | 116 (87.2) | 4 (3) | 13 (9.8) |
Dental check‑up | 85 (32) | 50 (18.8) | 131 (49.2) |
Lipid profile | 97 (40.2) | 93 (38.6) | 51 (21.2) |
TSH | 197 (90) | NA | 22 (10) |
Glucose (after the second step) | 107 (99.1) | NA | 1 (0.9) |
UACR | 176 (90.7) | NA | 18 (9.3) |
Orthopedic assessment | 43 (43.4) | 30 (30.3) | 26 (26.3) |
Psychological and psychiatric assessment (after the second stage)c | 186 (70.2) | 68 (25.7) | 11 (4.1) |
The highest number of adolescents with disorders that classified them as group 2 was found in the lipid profile assessment (38.6%), orthopedic assessment (30.3%), and in psychological and psychiatric assessment (25.7%) (Table 2). It is worth noting that almost 10% of adolescents had abnormal echocardiography with ECG results (group 3). In 1 patient, cardiac arrythmia (supraventricular extrasystoles) was detected. Diseases detected by echocardiography are presented in the Supplementary material, Tables S1 and S2.
The first step of blood glucose assessment showed elevated glucose values in 2.7% of adolescents; however, in the second step the percentage of abnormal results was 0. One child was qualified to group 3, despite lack of fasting blood glucose readings, because the parents reported in an interview that the child had diabetes (Table 2).
In addition, 71.7% of adolescents showed at least 1 borderline test result (group 2), and 75.7% of participants had at least 1 abnormal test result (group 3). Throughout the study, 315 incorrect test results were found, of which 14 (4.4%) were reported in interviews with parents.
This paper does not present the results of the biochemical tests for which the percentage of adolescents with abnormal values did not exceed 1%. This includes: serum C‑reactive protein, potassium and sodium levels, peripheral blood cell count, urinalysis, and urinary potassium and sodium levels.
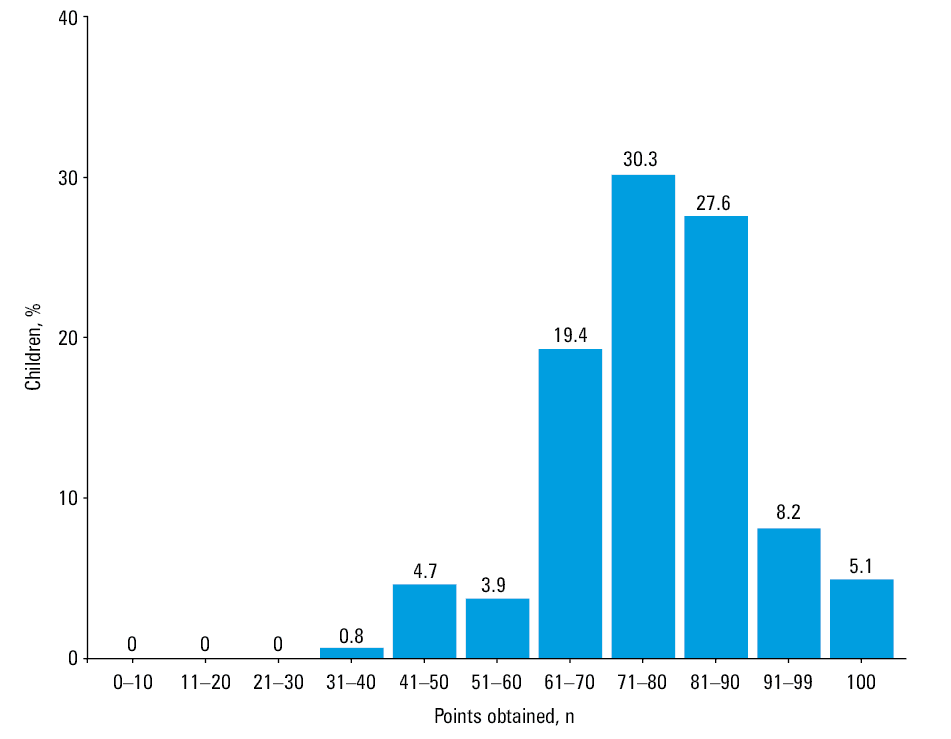
A total of 257 adolescents (91.1%) were included in a comprehensive health status analysis in which at least 5 groups of assessments were performed (Figure 1). Only 5.1% of children obtained a score of 100 points, which means that the results were within the age‑specific norm. The remaining 94.9% of participants received less than 100 points. After eliminating the medical examination in which the largest group of respondents was assigned to groups 2 or 3 (dental check‑up, 68% of teenagers), we observed that 12.2% of teenagers had all test results within the age‑specific norm.
Discussion
The results obtained in this study indicate a high prevalence of various health disorders and support the need to develop and implement an effective comprehensive screening model for adolescents. This will enable detection of disorders and early stages of diseases, and subsequently the implementation of appropriate education, prevention, diagnosis, and therapy. Such activities could lower the incidence of many future diseases.
Almost 24% of adolescents examined in our study were found to be overweight or obese. The problem of overweight and obesity in adolescents has become one of the main challenges for public health all over the world and is considered one of the most worrying health phenomena. In many countries, the incidence of obesity is an epidemic, also in adolescents and adolescents.13 In 2013, overweight and obesity affected 14.2% of children aged 5 to 17.9 years worldwide and it is expected that this proportion will increase to 15.8% in 2025.14 Importantly, global data are averaged and the scale of the problem differs significantly between countries—the percentages of overweight or obese children aged 5 to 17.9 years in Kiribati, Samoa, Micronesia, and Tonga in 2013 were as high as 56.9%, 46.1%, 45.6%, and 43.6%, respectively.14 According to data from the National Health and Nutrition Examination Survey performed in 2011 to 2012, overweight in the United States affects 34.2% of girls and 35.3% of boys aged 12 to 19 years, and obesity 30.6% of teenagers.15 An international report from the 2013 and 2014 survey in 15‑year‑old adolescents showed the highest prevalence of overweight and obesity in teenagers in Malta (26% of girls, 34% of boys), Greenland (29% of girls, 28% of boys), and Canada (21% of girls, 34% of boys). On the other hand, the lowest rates of overweight and obesity among teenagers were observed in Albania (5% of girls, 15% of boys), Armenia (6% of girls, 15% of boys), and Ukraine (6% of girls, 15% of boys). In this study, overweight and obesity concerned 7% of Polish girls and 22% of Polish boys, which was lower than the global average (13% for girls and 22% for boys).16 From the latest report from the HBSC study edited by Mazur and Małkowska‑Szkutnik,17 the problem of obesity and overweight concerns 8% of girls and 23.1% of boys. These data indicate a growing problem of overweight and obesity for Polish youth in this age group. It should be emphasized, however, that the reference values in the studies presented in the discussion were different than those in the current study. This comparison can be used for the preliminary estimation of the prevalence of obesity and overweight of Sopot youth in relation to the presented data. In our study, 24% of adolescents were found to be overweight or obese, which is a disturbing result and clearly indicates the need for anthropometric assessments in prevention programs. It was also shown that obesity in childhood not only increases the likelihood of obesity in adulthood, but that it is also closely related to the risk of developing cardiovascular diseases and diabetes.18,19 Moreover, Kasley et al20 showed that in people who were obese in childhood, health consequences may still be present despite the normalization of body weight.
In the present study, elevated BP values were found in every 10th teenager. Hypertension in children and adolescents is one of the most important health issues. It is an asymptomatic disease that, if untreated, leads to serious complications. Uncontrolled hypertension has serious direct and distant consequences, such as heart disease, stroke, atherosclerotic lesions, kidney disease, and blurred vision. In addition, the results of the NATPOL (Arterial hypertension and other CVD risk factors in Poland; Polish, Nadciśnienie tętnicze oraz inne czynniki ryzyka chorób serca i naczyń w Polsce) 2011 study clearly showed that the knowledge of Poles (aged 18–79 years) related to the criteria and complications of hypertension is insufficient.21 According to the experts of the European Society of Hypertension, measurement of BP should be part of a routine medical examination in children aged 3 years and older and in selected risk groups of children under 3.22 According to different authors, in the whole group of children and adolescents up to 18 years of age, the prevalence of hypertension is 2% to 5%, while in the group of teenagers it is higher and reaches 9% to 12%.23-26 The results of our study confirm the high incidence of elevated BP values, which is why it is important to emphasize the significance of BP measurements during each visit to a healthcare provider, also as part of a panel of prophylactic tests, and further diagnostics to detect secondary causes of hypertension.
Echocardiography and ECG assessment revealed cardiac abnormalities in over 13% of teenagers included in our study. Echocardiography is the basic diagnostic technique in cardiology characterized by high sensitivity; however, it is rarely used as a screening test due to high costs and the limited availability of equipment and qualified echocardiographers. It has been shown that this diagnostic method allows detection of abnormalities at every stage of a child’s life.27,28 The highest detectability of congenital defects is observed early in life. Severe defects are diagnosed and treated early. The detection rate of cardiac defects decreases with age. Some heart defects undergo spontaneous involution over time (eg, PFO, patent ductus arteriosus, muscular ventricular septal defect). However, some of the oligosymptomatic defects may be diagnosed by echocardiography in older children and even in adults (eg, atrial septal defect, moderate mitral regurgitation). Due to the increase in the number of children and adolescents engaged in intense sport activities, screening for cardiovascular diseases is important to detect abnormalities that are contraindications to sports or increase the risk of sudden death in athletes.29
In the present study, 3% of participants had mild abnormalities (group 2) which might worsen over time. Four adolescents were diagnosed with main pulmonary artery dilatation, bicuspid aortic valve (which predisposes to aortic valve stenosis or regurgitation), greater than physiological tricuspid regurgitation, and PFO (Supplementary material, Table S1).
Thirteen adolescents (9.7%) classified as group 3 were diagnosed with a total of 14 abnormalities (Supplementary material, Table S2). The most frequently reported pathological findings were moderate valve regurgitations, namely, mitral regurgitation (MI) in 8 patients and aortic valve insufficiency in 4 patients. In population‑based studies, mitral valve regurgitation occurs in 1% to 2.5% of patients.28-30 Valvular insufficiency cases detected in our study were of low grade and without hemodynamic significance. However, this defect can worsen with time. One child was diagnosed with ostium secundum atrial septal defect. This heart defect is oligosymptomatic and often without any abnormal findings in physical examination, and therefore remains undiagnosed or is diagnosed late. Screening tests allow its early detection and treatment. In one child, cardiac arrhythmia was detected thanks to simultaneous ECG recording. Further 12‑lead ECG revealed supraventricular extrasystoles. The child was recommended further diagnostics and follow‑up.
Screening echocardiography with ECG, although expensive and difficult to implement, is important for improving the health of children and adolescents and allow the detection, monitoring and, in selected cases, treatment of risk factors for cardiovascular diseases at an early stage of the child’s development. Therefore, if there are organizational and financial possibilities, it is beneficial to include echocardiography in the panel of screening tests for children and adolescents. Echocardiography should be preceded by ECG, or ECG can be performed simultaneously with echocardiography, to detect arrhythmias.
The dental assessment showed a high prevalence of caries (groups 2 and 3) (DMF >0) in teenagers in Sopot (68%). Tooth decay (dental caries) is a common disease. It is, next to periodontal disease, the main cause of the loss of teeth. The consequences of this process are serious disorders of the stomatognathic system that have a key impact on overall health.5 Data on the frequency of caries among 15‑year‑old adolescents in Poland from the research program implemented by the Ministry of Health, Monitoring of Oral Health in the Polish Population 2016–2020, indicate its very high prevalence that amounts to 94.9% in Mazowieckie Province, 94.5% in Dolnośląskie Province, and 92.5% in Lubelskie Province.31
According to a report by Mielnik‑Błaszczak et al,32 the prevalence of tooth decay among 15‑year‑old adolescents in the Podkarpackie Province is equally high and amounts to 96.67% for Nisko and 100% for Rzeszów. A study carried out in 2013 by the Health and Social Care Information Centre (NHS Digital) among 15‑year‑old students showed that percentages of adolescents with obvious decay experience were 44% in England and 63% in Wales.33 The frequency of caries in our study was 68%, which is a good result compared with data from the general Polish population. However, it should be emphasized that for many years, Sopot adolescents have been provided with dental care and dental offices are located in schools. Therefore, it seems that the lower prevalence of caries in children from Sopot compared with other cities in Poland may be caused by preventive and therapeutic activities by dental offices at schools. The epidemiological situation clearly indicates the need to introduce dental assessment into the basic panel of screening examinations.
Lipid metabolism disorders were found in almost 60% of the examined teenagers. Lipid disorders are often asymptomatic and may remain undiagnosed for decades, but they are one of the main risk factors for the occurrence of serious diseases such as heart attack, stroke, and kidney disease.34,35 In many epidemiological studies, it was shown that the elevated cholesterol level in childhood also persists into adulthood and is associated with an increased risk of cardiovascular disease.36,37 It has been shown that during puberty, LDL‑C levels decrease by 15% on average and false‑negative results may be obtained when diagnosing lipid disorders;38,39 therefore, the age of 9 to 11 years represents the best period for lipid metabolism assessment.40,41 Our study, despite the pubertal age of the participants, showed large deviations from the age‑specific norm, which is why it all the more indicates a major health problem among adolescents. These data clearly demonstrate that atherosclerosis prevention in both high‑risk and population‑based strategies should be started in childhood, ideally in accordance with the guidelines of the National Lipid Association Expert Panel on Familiar Hypercholesterolemia that recommend lipid profile assessment in all children aged 9 to 11 years.40,41 It seems that in children of this age, lipid levels should be measured as part of the screening program. The interpretation of test results in teenagers is difficult because there are no standards for Polish children and adolescents. The reference values adopted in our study are those recommended by the National Education Cholesterol Program, which are very general, gender independent, and same for children and adolescents. Zdrojewski et al42 showed that a significant percentage of young adult Poles aged 18 to 39 years have abnormal values of TC, LDL‑C, and TG (54.3%, 42.7%, 16.4%, respectively). In addition, Niklas et al43 showed a high prevalence of hypercholesterolemia and hypertension among young adults in the Polish population (age group 19–49 years, 15%). The high prevalence of lipid disorders in our study and the alarming epidemiological data for young adults indicate that lipid metabolism disorders are a serious health problem in Poland. It seems necessary to implement lipid profile assessment into the panel of screening test and develop reference values for Polish children and adolescents.
Abnormal TSH values were found in 10% of adolescents evaluated in our study. Analysis of TSH levels is challenging because there are no reference values developed specifically for Polish adolescents. What is more, there are no generally accepted reference values for children and adolescents in the world. In our analysis, we used reference values according to Kapelari et al10 in the form of centile charts. The magnitude of the problem showed by our study and the current state of knowledge on TSH clearly indicates that a TSH test should be implemented in screening programs. At the same time, it is necessary to develop reference values for Polish adolescents.
Two‑step screening blood glucose assessment revealed no patient with elevated glycemic values. One child was qualified to group 3 for blood glucose levels (Table 2) because the interview with parents revealed that their child was diagnosed with diabetes at the age of 10 years. It should be emphasized that in fasting blood glucose testing, it is crucial to verify this parameter in people whose results after the first determination are above the reference values. In our study, 2.7% of adolescents have elevated fasting blood glucose in the first step of blood glucose assessment; however, after repeating the instructions regarding proper preparation for the test, the measurements in this group of adolescents were normal. It should also be remembered that the most common form of diabetes in juvenile Caucasian patients is type 1 diabetes, which is characterized by numerous and very dynamic clinical symptoms. These arguments raise the question about the need for blood glucose measurement in screening panel for adolescents. Szczerbiński et al44 suggested that physical activity may serve as a protective factor against type 2 diabetes, therefore it is worth implementing such prevention methods in adolescents.
In the present study, almost 10% of adolescents had elevated UACR. Albuminuria is a recognized indicator of not only kidney damage but also vascular endothelium dysfunction in patients with hypertension, diabetes and/or cardiovascular diseases.45-47 Albuminuria was used for early detection of chronic kidney disease in an adult population and was found to occur at a surprisingly high rate. In the PolNef (Program for Early Detection of Chronic Kidney Disease in Poland) study, albuminuria was detected in 11.9% of the study population.48 Our previous study in the adolescent population showed that more than 11% had elevated UACR.49 In the present study, 9.3% of adolescents had UACR higher than 30 mg/g. This confirms the surprisingly high incidence of albuminuria at such a young age. However, the lack of albuminuria cannot be the basis to exclude nephropathy. Adolescents with albuminuria should be followed‑up to monitor kidney function. The high prevalence of elevated UACR indicates the need to include this parameter into the screening panel.
Results of the orthopedic assessment showed that 30% of adolescents require prophylaxis to prevent postural defects, and 26% require further diagnostics and potential treatment. A child’s poor posture, and especially planovalgus foot, is one of the frequent reasons for the parents’ anxiety and, consequently, visits to pediatricians and orthopedists. Until today, no uniform management standard has been adopted and this applies to diagnostic methods, classification, prevention and treatment. Only physical examination can be used for screening purposes. Footprint analysis is also not entirely reliable, depending on the technique used, while at the same time, this examination significantly extends the time and increases the cost of the entire orthopedic assessment.50
Currently, the vast majority of researchers focus on the functional aspect, that is, the dynamics of the lower limb as the main factor responsible for potential pathology.51 Hence, in our study, particular emphasis was put on assessing the dynamics of the musculoskeletal system. This approach was aimed at distinguishing a symptomatic planovalgus foot (uncorrectable, painful, or conflicting with footwear) as the only pathology requiring intervention, leading to the development of biomechanical disorders of the musculoskeletal system, especially the lower limb and the spine.51-53 There is a significant discrepancy in the literature regarding the prevalence of flat feet in adolescents aged 14 years. In studies conducted in Africa and the Middle East, the prevalence rate was 12% to 13%, while in European studies, it was 46% to 50%.50,53 At the same time, in all studies, the rates of symptomatic flat foot (if such a category was created) did not exceed several percent.50,52 This discrepancy may indicate both the lack of objective research methods and differences between study populations in terms of race, weight, or lifestyle.
Considering the fact that the vast majority of research centers around the world report the self‑improvement of the valgus deformity of feet up to the age of 10 years, it seems reasonable to carry out such screening tests in younger children, between 10 and 12 years of age.
The psychological and psychiatric assessment revealed depressive symptoms in 25.6% of examined population, and 4.1% of adolescents were diagnosed with clinical depression. Depression is one of the most serious health and social problems in the world. It is a quite rare disorder in prepubertal children, but with the onset of adolescence its frequency remarkably increases and remains at a high level afterwards. The prevalence of clinical depression in young children is 1% to 2% and in the first phase of adolescence it increases and reaches 3% to 8%, whereas the prevalence in the whole period from childhood to the end of adolescence is 20%.54-56 In a recent study in a cohort of Polish 15‑year‑old teenagers, depressive symptoms occurred in 27.4% of girls and 19.2% of boys.57 A similar, although slightly higher, result was obtained in the SOPKARD‑Junior study—the prevalence of depressive symptoms in students of junior high schools in Sopot was 29.7%. In the SOPKARD‑Junior program, apart from the assessment of the severity of depressive symptoms, psychiatric verification of the diagnosis was carried out based on medical criteria. The prevalence of depression among teenagers from Sopot (4.1%) does not differ significantly from the prevalence of this disorder in other parts of the world, although the rates of depression in American teenagers are even higher.58 A striking result of the SOPKARD‑Junior program is the high percentage of adolescents at risk (risk group), that is, every third teenager had depressive symptoms. These adolescents may develop clinical disorders in the future that would require treatment; therefore, early education and prevention addressed to this group of young people would be of particular importance. One in twenty 14‑year‑old children had clinical depression, which suggests that in every class at junior high schools there may be a child with depression who requires specialist treatment and help. This health situation clearly indicates the need to introduce a 2‑step psychological‑psychiatric examination, that is, questionnaire surveys to identify a group of adolescents with depressive symptoms (the first step) and visits of this group of adolescents at a child psychiatrist in order to verify and possibly confirm the diagnosis of depression (the second step).
The additional goal of the study was to propose a panel of screening assessments based on the epidemiological situation of adolescent health in a selected urban population, which should be included in the prevention program. Obviously, determining the actual state of health through medical diagnosis is crucial to establishing an appropriate preventive approach, but it cannot be the only factor that influences the selection of tests to be performed as part of screening programs. The cost‑effectiveness ratio as well as the availability of qualified staff, medical equipment, and space are also important. In this study, a comprehensive health analysis based on a holistic assessment of teenagers’ health using a burden analysis showed that only 5.1% of participants scored 100 points. This means that in this group of teenagers, all medical examination results were within the age‑specific norm. The lower the score obtained in the analysis, the poorer the health status. Adolescents with lower score require more intensive preventive and therapeutic activities (Figure 1). A score of less than 100 points was obtained by as many as 94.9% of adolescents. This means that in this group of adolescents there are at least borderline or abnormal results. This group of almost 95% of adolescents requires education, prevention and treatment, as the progression of the detected disease and/or risk factors is associated with negative, often irreversible health consequences. As many as 71.7% of respondents were classified at least once into a group with a borderline result (group 2). This means that these adolescents should be provided with regular diagnostic workup and education. The fact that 75.7% of patients were diagnosed with a disease/abnormal result (group 3) is worrying. Out of 315 diagnosed disease/abnormal result entities, only 14 (4.4%) were reported by parents in interviews, which means that parents’ awareness of the health status of their adolescents is very poor.
This disturbing health situation of adolescents clearly indicates very high needs in the area of education, prevention, and treatment in this population. The prevalence of borderline results and diseases/abnormal result found in the anthropometric, BP, echocardiographic, ECG, dental, orthopedic, psychological‑psychiatric, lipid profile, TSH, and UACR assessments indicates that all these tests should be included in prevention programs dedicated to adolescents. The implementation of prevention of many disorders and diseases in adolescents is too late. It seems reasonable that this screening panel should be implemented in younger children in order to reduce the prevalence of risk factors and diseases in adolescence.
In order to plan interventions and issue recommendations on the range of screening tests included in the model preventive program for all Polish adolescents, it is necessary to perform a full range of assessments carried out in the SOPKARD‑Junior Program in various regions of Poland. Our study certainly indicates that the needs are large, and extensive educational, preventive, and therapeutic activities should be implemented for this part of the population throughout Poland.
Conclusions
A large number of adolescents diagnosed with borderline value, or abnormal result/disease and comprehensive health analysis clearly indicates high needs in the area of prevention and treatment in adolescents. Therefore, it is necessary to develop a model of comprehensive screening assessment. Moreover, our study indicates that anthropometric (BMI), arterial BP, echocardiographic, ECG, dental, orthopedic, psychological‑psychiatric, lipid profile, TSH, and UACR assessments should be included in the standard screening panel for adolescents. The large number of adolescents with lipid metabolism disorders (according to the American reference values) and abnormal TSH levels (according to the Austrian reference range) indicates that there is a need to develop reference values of these parameters for Polish adolescents and objectively verify these disorders.
- World Health Organization. Programming for adolescent health and development: report of WHO/UNFPA/UNICEF study group on programming for adolescents health. Geneva: World Health Organization; 1999.
- Suligowska K, Czarniak P, Krawczyk M, et al. An assessment of health status and health behaviours in adolescents: main points and methods of the SOPKARD‑Junior programme. Arch Med Sci. 2018; 14: 38‑51. | Crossref
- Kułaga Z, Litwin M, Tkaczyk M, et al. Polish 2010 growth references for school‑aged children and adolescents. Eur J Pediatr. 2011; 170: 599‑609. | Crossref
- Kułaga Z, Litwin M, Grajda A, et al, Grupa Badaczy OLAF. Distribution of blood pressure in school‑aged children and adolescents reference population . Stand Med Pediatr. 2010; 7: 100‑111.
- Jańczuk Z. Stomatologia zachowawcza. Zarys kliniczny. Wydawnictwo Lekarskie PZWL; 2008; 162‑170.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION