Severe acute respiratory syndrome coronavirus 2 pneumonia and pulmonary embolism in a 66-year-old woman



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Severe acute respiratory syndrome coronavirus 2 pneumonia and pulmonary embolism in a 66-year-old woman
Elevated levels of D‑dimer are discussed as a marker for an unfavorable outcome in severe acute respiratory syndrome coronavirus 2 infections. Zhang et al1 reported significantly higher levels of D‑dimer (as well as C‑reactive protein and procalcitonin) as associated with a more severe course of the disease in an analysis of the records of 140 hospitalized patients with coronavirus disease 2019 (COVID‑19). The authors discussed the elevated D‑dimer levels as indicative of a sustained inflammatory response and disturbed coagulation after the infection. Other authors confirmed that elevated D‑dimer levels are a negative prognostic factor, for example, Zhou et al2 in a retrospective multicenter cohort study in 191 patients.
So far, there is limited data on whether SARS‑CoV‑2 infection also favors thromboembolic events. Danzi et al3 recently reported the case of a 75‑year‑old patient (sinus rhythm on electrocardiogram) with a severe bilateral SARS‑CoV‑2 pneumonia and concomitant acute pulmonary embolism (no strong predisposing risk factors for venous thromboembolism). Xie et al4 also reported 2 cases from Wuhan (57- and 70‑year‑old men) in which SARS‑CoV‑2 pneumonia was complicated by acute pulmonary embolism. Coronavirus disease 2019 with changes in the lung could theoretically induce a hypercoagulable state. The vascular response to (systemic) hypoxia is controlled by hypoxia‑inducible transcription factors. The target genes of hypoxia‑inducible transcription factors include factors regulating thrombus formation.5
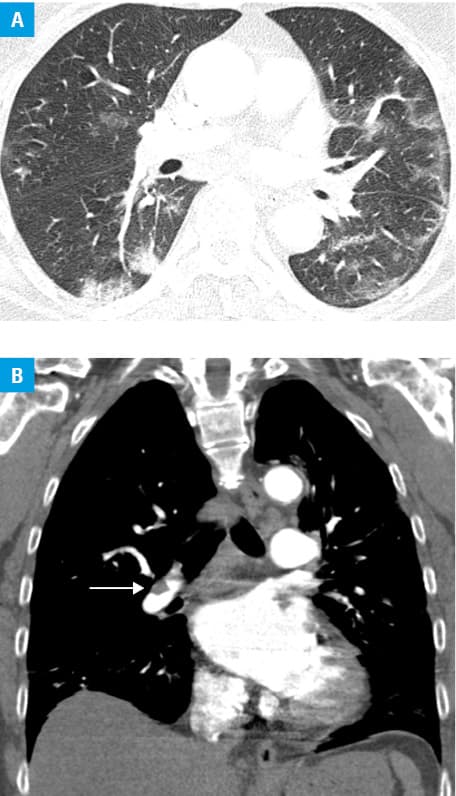
We report the case of a 66‑year‑old woman who tested positive for COVID‑19 one week before the admission. She was admitted to our clinic due to atrial fibrillation and because she felt as if she was about to faint (March 31, 2020). Furthermore, she complained of a light cough and rhinitis; she had no fever. For about 3 months, she had had recurrent infections of the upper respiratory tract and reported loss of taste. She did not complain of chest pain and was hemodynamically stable. It could not be clarified whether the atrial fibrillation was a new‑onset pathology or (very likely) a rather long‑standing disorder. Otherwise, the patient was healthy, she was not hypertensive and did not have diabetes mellitus or thyroid disorders nor was she obese (body mass index, 25.2 kg/m2). We determined D‑dimer levels for risk stratification of the severity of the disease and found they were elevated at 14903 µg/l (reference range <230 µg/l). C‑reactive protein levels were elevated with 95.9 mg/l (reference range <5 mg/l), procalcitonin levels were normal. Thus, we performed an unenhanced computed tomography scan of the thorax (Figure 1A) as well as computed tomography pulmonary angiography (Figure 1B). Bipulmonary ground‑glass opacities with transition to consolidations compatible with COVID‑19 viral pneumonia could be visualized. The imaging also demonstrated pulmonary arterial emboli on both sides in the lower lobes. Further, genetic risk factors such as loss of function mutations (deficiencies of antithrombin, protein C, protein S) and gain of function mutations (such as prothrombin mutation G20210A, factor V Leiden) were excluded and the patient was treated with apixaban. She was discharged on April 3, 2020. A specific therapy of the SARS‑CoV‑2 pneumonia, apart from inhalations, was not required.
Our as of yet limited database allows no conclusions about an elevated risk for pulmonary embolism in patients with SARS‑CoV‑2 pneumonia and with preexisting risk factors for such events as present in the current case. Analyzing the datasets of Zhou et al,2 D‑dimer levels were about 10‑fold higher in the nonsurvivor group. In the case reported here, D‑dimer levels were 65‑fold higher. The case exemplifies that the presence of elevated D‑dimer levels should not only be regarded as a risk factor for an unfavorable course of SARS‑CoV‑2 pneumonia but should also prompt physicians to exclude pulmonary embolism in patients with established risk factors for such events.
- Zhang JJ, Dong X, Cao YY, et al. Clinical characteristics of 140 patients infected with SARS‑CoV‑2 in Wuhan, China. Allergy. 2020 Feb 19. . | Crossref
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID‑19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395: 1054‑1062. | Crossref
- Danzi GB, Loffi M, Galeazzi G, Gherbesi E. Acute pulmonary embolism and COVID‑19 pneumonia: a random association? Eur Heart J. 2020 Mar 30. . | Crossref
- Xie Y, Wang X, Yang P, Zhang S. COVID‑19 complicated by acute pulmonary embolism. Radiology: Cardiothoracic Imaging. 2020; 2: e200067. | Crossref
- Gupta N, Zhao YY, Evans CE. The stimulation of thrombosis by hypoxia. Thromb Res. 2019; 181: 77‑83. | Crossref
ARTICLE INFORMATION