Atypical course of infective endocarditis in a patient with complex congenital heart disease, chronic hepatitis B virus infection, and splenic marginal zone lymphoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atypical course of infective endocarditis in a patient with complex congenital heart disease, chronic hepatitis B virus infection, and splenic marginal zone lymphoma
We present a case of a 25‑year‑old man with complex congenital heart disease: dextrotransposition of the great arteries, ventricular septal defect, double outlet right ventricle, coarctation of the aorta, hypoplastic aortic arch, patent ductus arteriosus, status post multistage cardiac surgery (the Rashkind procedure, the Senning procedure, excision of subvalvular muscular stenosis of the pulmonary artery), thymectomy, pacemaker implantation at the age of 4 years, chronic hepatitis B virus infection (diagnosed in the first year of life), currently on Entecavir (lamivudine) therapy.
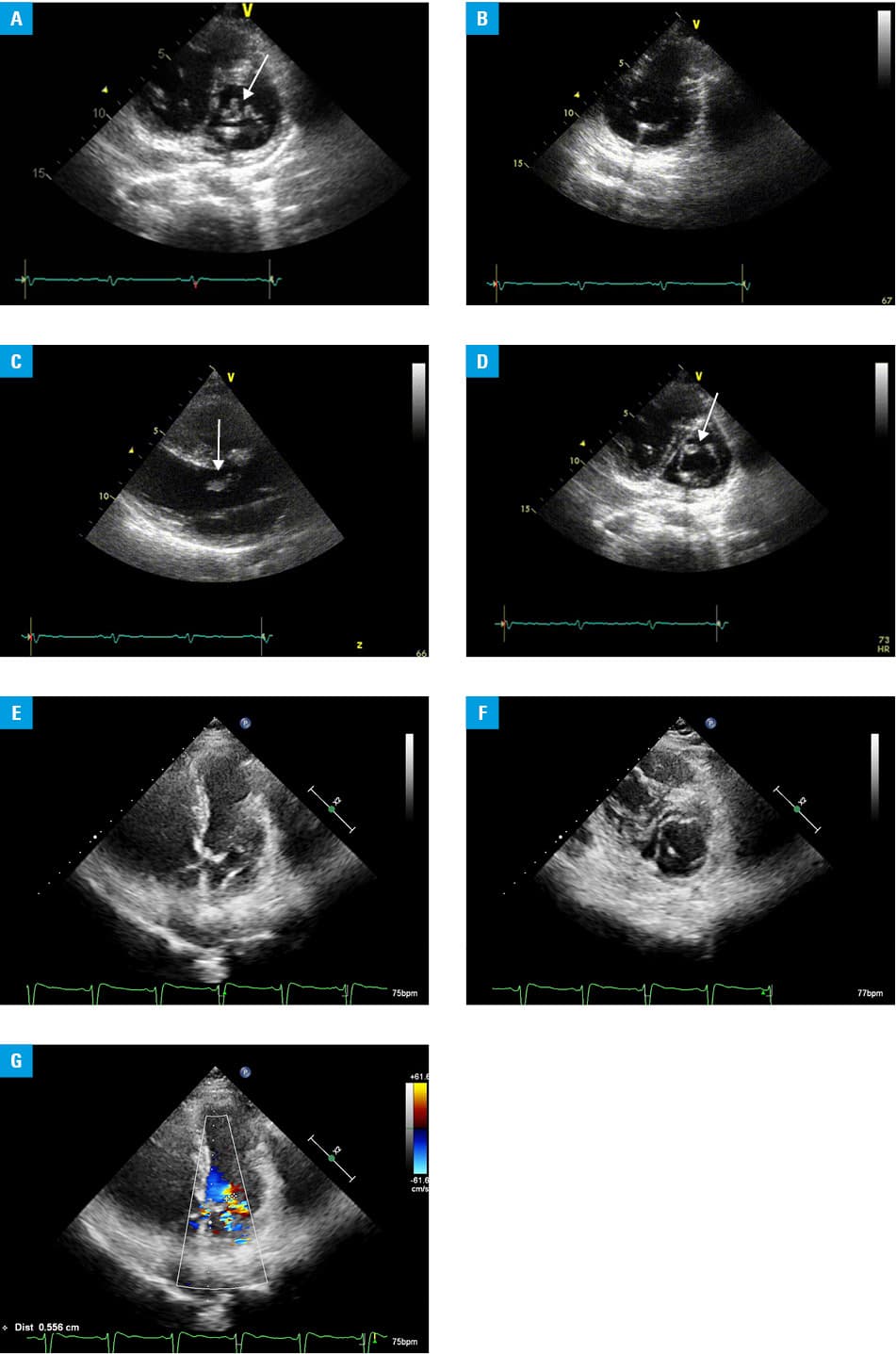
The patient was admitted to the cardiology department due to suspicion of infective endocarditis. Persistent signs and symptoms included: dry cough, dyspnea, fever of up to 40 °C, weakness, and increased sweating. He was treated with various antibiotics for months. Blood culture did not reveal any pathogens. Echocardiography showed reduced myocardial contractility and mobile, echodense masses (Figure 1A–1D). Scintigraphy demonstrated infective endocarditis at pacemaker electrodes and an increased marker accumulation in the liver and the spleen (Supplementary material, Figure S1). The electrodes were replaced after the diagnosis had been established.
During hospitalization, blood test results were as follows: white blood cells, 18 × 109/l; lymphocytes, 43%; hemoglobin, 12.6 g/dl; and platelets, 65 × 109/l. On blood smear, 17% of atypical lymphoid cells with villi were found. The patient tested negative for hepatitis C virus. On physical examination, the lymph nodes, the spleen, and the liver were not enlarged. Flow cytometry of peripheral blood lymphocytes showed 22% of monoclonal B lymphocytes: CD19+/CD22+, CD20bright, FMC7+ bright, IgM+ bright/CD43+/CD11c+/CD52+/CD58+/kappa+ /CD38–/CD5–/CD23–/CD71–/CD10–/CD25– /CD103–/kappa–/CD138–, which was indicative of indolent lymphoma. Ultrasonography of the abdomen revealed the slightly enlarged spleen, 135 × 52 mm in size. Two trephine biopsies, taken during hospitalization and after 6 months, revealed a small population of B cells in an atypical localization, but lymphoproliferative disease was not confirmed. The spleen was removed owing to its rapid enlargement reaching 231 mm × 85 mm.
Histological examination of the spleen and lymph nodes showed an atypical, obliterated structure of the spleen. Finally, splenic marginal zone lymphoma (SMZL) was diagnosed with minimal hemophagocytosis in the spleen and the adjacent lymph nodes. The coexistence of SMZL and hemophagocytic syndrome was excluded based on laboratory test results. Computed tomography of the abdomen and the pelvis showed the lymph nodes of 30 mm in diameter. The patient did not receive any directed treatment immediately after the onset of symptoms, because histological examination did not confirm the diagnosis. Eventually, the patient was treated with 4 doses of rituximab (375 mg/m2 once a week). His abdominal ultrasound after treatment was normal and blood count was also normalized. Echocardiography performed after 2 years revealed good contractility and no signs of inflammation (Figure 1E–1G).
Splenic marginal zone lymphoma affects mainly elderly or middle‑aged patients at a median age of 65 years. Here, we described a case of one of the youngest patients with SMZL reported in the literature.1,2
Neoplasms such as lymphoma may be the cause of an atypical course of infective endocarditis.3-5 Oncologists and hematologists should be aware of potential complications of their patients’ cardiovascular status, such as infective endocarditis, and refer them to a cardiologist if cardiac symptoms are observed.
- Depowski PL, Dunn H, Purdy S, et al. Splenic marginal zone lymphoma: a case report and review of the literature. Arch Pathol Lab Med. 2002; 126: 214‑216.
- Perrone S, D’Elia GM, Annechini G, et al. Splenic marginal zone lymphoma: prognostic factors, role of watch and wait policy, and other therapeutic approaches in the rituximab era. Leuk. Res. 2016; 44: 53‑60. | Crossref
- Fernández‑Cruz A, Muñoz P, Sandoval C, et al. Infective endocarditis in patients with cancer: a consequence of invasive procedures or a harbinger of neoplasm?: a prospective, multicenter cohort. Medicine (Baltimore). 2017; 96: e7913. | Crossref
- Murdoch DR, Corey GR, Hoen B, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis‑Prospective Cohort Study. Arch Intern Med 2009; 169: 463‑473. | Crossref
- Kyu K, Darae K, Sang‑Eun L, et al. Infective endocarditis in cancer patients – causative organisms, predisposing procedures, and prognosis differ from infective endocarditis in non‑cancer patients. Circ. J. 2019; 83: 452‑460. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION