Nicotinamide adenine dinucleotide phosphate (NADPH) oxidase p22phox subunit polymorphisms, systemic oxidative stress, endothelial dysfunction, and atherosclerosis in type 2 diabetes mellitus
Key words: atherosclerosis, cytochrome b-245 alpha chain (CYBA) polymorphisms, diabetes mellitus, endothelial function, nicotinamide adenine dinucleotide phosphate (NADPH) oxidases



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Nicotinamide adenine dinucleotide phosphate (NADPH) oxidase p22phox subunit polymorphisms, systemic oxidative stress, endothelial dysfunction, and atherosclerosis in type 2 diabetes mellitus
Introduction: Diabetes mellitus is an important and rapidly increasing problem in public health. It is associated with endothelial dysfunction and increased endothelial permeability, which may lead to severe cardiovascular events.
Objectives: We aimed to evaluate the relationship between polymorphisms of the cytochrome b‑245 alpha chain (CYBA) gene encoding p22phox, a key subunit of nicotinamide adenine dinucleotide phosphate oxidase, and endothelial function, atherosclerosis, and systemic oxidative stress in type 2 diabetes mellitus (T2DM).
Patients and methods: Intima‑media thickness as well as flow- and nitroglycerin‑mediated dilatation were measured in 182 patients with T2DM. Assessment of plasma levels of von Willebrand factor and malondialdehyde as well as genotyping of the coding sequence C242T (rs4673) and promoter region A‑930G (rs9932581) polymorphisms of CYBA were performed using standardized protocols.
Results: We observed a significant association of the impaired endothelial function, as measured by flow‑mediated dilatation, with the C allele of the C242T polymorphism, but not with the A‑930G polymorphism. Functional relationship of the C242T polymorphism with endothelial dysfunction remained significant following a multivariable adjustment for major risk factors for atherosclerosis. Mean intima‑media thickness, nitroglycerin‑mediated dilatation, and concentrations of malondialdehyde or von Willebrand factor were not related to the specific genotypes of the investigated polymorphisms.
Conclusions: The C242T polymorphism of the CYBA gene significantly affects endothelial function in T2DM, whereas the A‑930G polymorphism does not. Thus, the former might be a useful marker of endothelial dysfunction in patients with T2DM.
What's new?
The current study found a protective effect of the T allele of the missense rs4673 polymorphism of the cytochrome b‑245 alpha chain (CYBA) gene, encoding the p22phox subunit of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase, on flow‑mediated dilatation in patients with type 2 diabetes mellitus. A growing body of evidence suggest that this particular genetic variation may have important phenotypic consequences in diseases related to endothelial function and redox balance, such as diabetes and cardiovascular diseases.
Introduction
Diabetes mellitus is an important and rapidly increasing worldwide problem. In 2013, there were approximately 382 million of people with diabetes mellitus and 90% to 95% of them had type 2 diabetes mellitus (T2DM).1,2 Diabetes contributes to endothelial dysfunction, increased endothelial permeability, atherosclerosis, as well as disturbance of the epicardial transcriptomic profile and thus may lead to severe cardiovascular events, including myocardial infarction and stroke.3-5
Hyperglycemia causes alterations in the cellular redox state and leads to increased production of reactive oxygen species (ROS).6 Additionally, autoxidation of glucose and oxidation of glycated protein fragments may be a source of significant amounts of ROS and lead to cellular injury.7 The main vascular sources of superoxide anion are enzymes of nicotinamide adenine dinucleotide phosphate (NAPDH) oxidase (NOXs) and dysfunctional endothelial nitric oxide synthase (eNOS).8 Recent studies have demonstrated a stimulating effect of glucose and advanced glycation end‑products on NOX activity.9,10 High glucose concentration induces NOX expression and superoxide anion production in human endothelial cells, leading to endothelial dysfunction.11 Superoxide anion exaggerates oxidation processes, including oxidation of polyunsaturated fatty acids in low‑density lipoprotein (LDL) particles, which promotes atherosclerosis. Numerous clinical studies have shown that NOX activity correlates with various risk factors for atherosclerosis, including T2DM.8
The NOX complex consists of 2 membrane subunits, p22phox and gp91phox / NOX2 (or one of its homologues—NOX1, NOX3, NOX4, or NOX5), 3 cytoplasmatic subunits (gp67phox, p47phox, and p40phox), and a G‑protein (Rac).12 While vascular subunits associated with p22phox—NOX1 and NOX2—are thought to have a deleterious effect on the cardiovascular system due to inactivation of nitric oxide (NO), the role of NOX4 is more complex.13 The presence of the p22phox subunit is crucial for enzyme activity, and 2 polymorphisms of this gene, that is, C242T in the coding region (which changes histidine‑72 to tyrosine) and A‑930G in the promoter region, have been intensively studied as modulators of oxidative stress and atherosclerosis progression.14-20 Importantly, the functional consequences of genetic polymorphisms may be revealed particularly under “stress” conditions, that is, in the presence of factors that overload the cardiovascular system, such as T2DM.21
The present study aimed to evaluate the relationship between the missense C242T (rs4673) and promoter region A‑930G (rs9932581) polymorphisms of the p22phox subunit of NOXs, encoded by the cytochrome b‑245 alpha chain (CYBA) gene, and clinically assessed endothelial function and atherosclerosis progression, as well as biochemical parameters related to endothelial function and systemic oxidative stress in patients with T2DM.
Patients and methods
Study participants and definitions
A total of 182 White patients diagnosed with T2DM (see Table 1 for detailed clinical characteristics and medications used in the study cohort) were consecutively enrolled and followed up at the Department of Metabolic Diseases of the University Hospital in Kraków, Poland. Detailed medical history and physical examination of all patients were described previously.22,23 In particular, 71, 30, and 62 patients presented microangiopathic complications related to diabetic retinopathy, nephropathy, and / or neuropathy, respectively. Diabetes was diagnosed according to the criteria of the World Health Organization.24,25 To maximize homogeneity of the study group, we included patients with T2DM who were over 30 years old and in whom diabetes was diagnosed at least 2 years earlier. Hypertension was defined as antihypertensive treatment or systolic blood pressure greater than or equal to 140 mm Hg and / or diastolic blood pressure greater than or equal to 90 mm Hg. Dyslipidemia was defined as total cholesterol level exceeding 5 mmol/l or level of triglycerides exceeding 1.7 mmol/l or level of LDL cholesterol greater than 1.8 mmol/l.26,27 Peripheral blood for DNA isolation and assessment of biochemical parameters was obtained by antecubital vein puncture. The study was approved by the Jagiellonian University Bioethics Committee. All patients provided informed consent to participate.
Parameter | Value |
Abbreviations: BMI, body mass index; FMD, flow‑mediated dilatation; HbA1c, glycated hemoglobin; HDL, high‑density lipoprotein; IMT, intima‑media thickness; IQR, interquartile range; LDL, low‑density lipoprotein; NMD, nitroglycerin‑mediated dilatation | |
Clinical characteristics | |
Age, y, mean (SD) | 56 (7) |
Male sex, n (%) | 91 (50) |
Arterial hypertension, n (%) | 161 (88.4) |
Dyslipidemia, n (%) | 179 (98.3) |
Ischemic heart disease, n (%) | 86 (47.2) |
History of myocardial infarction, n (%) | 22 (12.1) |
Obesity (BMI ≥30 kg/m2), n (%) | 109 (59.8) |
BMI, kg/m2, mean (SD) | 32.7 (6.5) |
Microangiopathic complication, n (%) | 104 (57.1) |
Current smoking, n (%) | 39 (21.4) |
FMDmax, %, median (IQR) | 8.8 (6–12.3) |
NMDmax, %, median (IQR) | 15.2 (11.8–18.9) |
IMTmean, mm, median (IQR) | 0.84 (0.73–0.93) |
Biochemical parameters, median (IQR) | |
Total cholesterol, mmol/l | 5.1 (4.5–5.9) |
LDL cholesterol, mmol/l | 2.9 (2.4–3.6) |
HDL cholesterol, mmol/l | 1.1 (1–1.3) |
Triglycerides, mmol/l | 1.9 (1.4–2.9) |
C‑peptide, mg/ml | 3.0 (1.7–4) |
Creatinine, µmol/l | 75.3 (65.7–87.6) |
HbA1c, % | 7.6 (6.8–8.8) |
Treatment or medication use, n (%) | |
Only diabetic diet | 13 (7.1) |
Oral antidiabetic medication | 115 (63.2) |
Insulin | 96 (52.7) |
Angiotensin converting enzyme inhibitor | 140 (76.4) |
Diuretic | 91 (50) |
Statin | 90 (49.5) |
Acetylsalicylic acid | 79 (43.4) |
β-Blocker | 67 (36.3) |
Calcium channel blocker | 43 (23.1) |
Nitrate | 27 (14.8) |
α-Blocker | 14 (7.7) |
Genotyping and biochemical tests
DNA was isolated using the QiaAmp Mini Blood Kit (QIAGEN, Hilden, Germany) according to the manufacturer’s recommendations. DNA amplification was performed using the T3 Thermocycler (Biometra, Göttingen, Germany) and Hot Star Taq Polymerase (QIAGEN). The following primer pairs were used for amplification: for C242T, FW‑5’-TGCTTGTGGGTAAACCAAGGCCGGTG‑3’ and RV‑5’-AACACTGAGGTAAGTGGGGGTGGCTCCTGT‑3’28 and for A‑930G, FW‑5’-AAACCACCAAGTGCCTCGGATGGTGGCT‑3’ and RW‑5’-CCAGCGCCCATGGGAAGACTTTAGACCT‑3’. Polymerase chain reaction (PCR) consisted of 15‑minute denaturation (95 ºC), 40 cycles of denaturation (94 ºC/45 s), annealing (60 ºC/45 s), elongation (72 ºC/45 s) and final 10‑minute elongation (72 ºC). Products of PCR were subsequently incubated with restriction enzymes, RsaI (Fermentas, Burlington, Ontario, Canada; 0.1 U/µl; 37 ºC/16 h) or BbvI (Fermentas, 0.06 U/µl, 65 ºC/16 h) to identify genotypes of the coding sequence (C242T) or promoter region (A‑930G) polymorphisms, respectively. Identification of genotypes was performed following agarose gel electrophoresis by 2 independent researchers in the following way: 348 bp band (allele C) and 160 + 188 bp bands (allele T) for the C242T polymorphism and 318 bp band (allele A) and 232 bp band (allele G) for the A‑930G polymorphism.
Standard laboratory tests including glucose level, lipid profile as well as creatinine, C‑peptide, and glycated hemoglobin levels were performed. Measurement of plasma levels of von Willebrand factor (vWF) was performed with Enzyme‑Linked Immunosorbent Assay (ELISA) utilizing rabbit antibodies (DAKO, Glostrup, Denmark). Assessments of malondialdehyde (MDA) plasma levels were performed by a modified method described by Sim et al29 using high‑performance liquid chromatography–mass spectrometry (LCQ Finnigan Matt; Adaptas SIS, Palmer, Massachusetts, United States). Samples were incubated with sodium hydroxide to liberate the bound MDA and with perchloric acid to precipitate proteins. Afterwards, the supernatant was extracted 2 times with n‑hexane and the organic phase was analyzed.
Clinical tests
Flow‑mediated dilatation (FMD)was evaluated as a marker of endothelial function through the measurement of brachial artery diameter before and after acute 5‑minute occlusion (with a sphygmomanometer cuff) using techniques consistent with the guidelines,30 as described and validated before.31 Briefly, assessments were performed with a Toshiba Xario Ultrasound System SSA‑340A ultrasonograph, type BF (Toshiba, Tokyo, Japan) and a 8‑MHz linear transducer. Before the examination, patients were placed in a supine position for 15 minutes in a calm and darkened room. The right arm was immobilized and a blood pressure cuff was placed and inflated around it to at least 200 mm Hg in order to achieve brachial artery occlusion for 5 minutes. Diastolic measurements were performed before cuff inflation and then subsequently 1, 2, and 5 minutes after cuff deflation.
Nitroglycerin‑mediated dilatation (NMD) was measured to investigate non–endothelium‑dependent vasodilation. Vessel diameter was assessed before and 1, 2, and 5 minutes after sublingual application of 400 µg of nitroglycerin. Vessel diameter was measured as a distance between 2 M‑lines, according to the original Celermajer’s methodology.32 Maximum FMD (FMDmax) and NMD (NMDmax) were calculated as 100 × (peak vascular diameter after hyperemia or nitroglycerin application – baseline vascular diameter) / baseline vascular diameter.33,34
Intima‑media thickness (IMT) measurements were performed using the standard method and the same device as described previously.31 Briefly, assessments were performed at 12 different points on the right and left common carotid arteries, measuring the distance between the border between the artery lumen and carotid artery intima and the second bright M‑line (the border between the media and adventitia). On the basis of the measurements, the mean and maximum IMT (IMTmean and IMTmax) were calculated.
Statistical analysis
Correlations between 2 continuous variables were evaluated by the Spearman test, while associations between categorical variables were tested using the Pearson’s χ2 test. Differences between the genotypes, as well as recessive and dominant effects of the analyzed single‑nucleotide polymorphisms (SNPs), were tested using the Kruskal–Wallis and Mann–Whitney tests, respectively. Logistic regression was used to test the effect of SNPs on dichotomized FMDmax (based on the median value) or ischemic heart disease with additional adjustment for potential confounders. Concordance of the genotypes with the Hardy–Weinberg equilibrium was tested with the Pearson’s χ2 test. A significance level of P less than 0.05 was assumed for statistical tests. Statistical analyses were performed using Statistica (version 7.1; Stat Soft, Inc., Tulsa, Oklahoma, United States) and SPSS (version 25.1; IBM Corp, Armonk, New York, United States).
Results
Patients’ characteristics
The study group included 182 patients with T2DM (Table 1). The most common risk factors for atherosclerosis among the investigated patients were hypertension and dyslipidemia, while ischemic heart disease was diagnosed in nearly half of the subjects (Table 1). As expected,31 we observed a negative correlation between mean IMT and maximal FMD, which provided additional validation of our protocol (R = –0.44; P <0.001). Interestingly, a significant correlation between maximal NMD and mean IMT (R = –0.37; P <0.001) was observed as well.
Association between CYBA gene polymorphisms and intima media thickness, endothelial function, or ischemic heart disease
Based on the frequencies of minor T242 and A‑930 alleles (37.9% and 39.8%, respectively), the studied SNPs were common in the T2DM population. Distribution of both polymorphisms did not significantly deviate from the one expected based on the Hardy–Weinberg equilibrium. Moreover, no linkage disequilibrium was observed between the C242T and A‑930G polymorphisms (D’ = 0.12; R2 = 0.005).
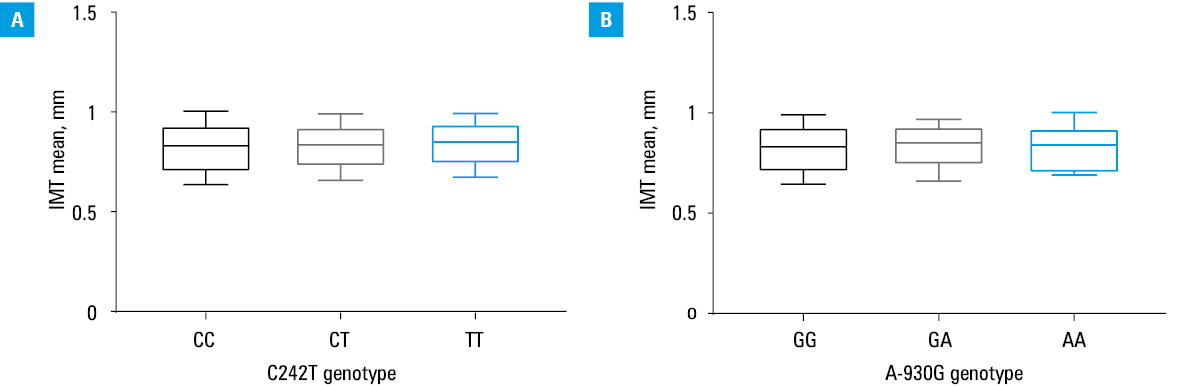
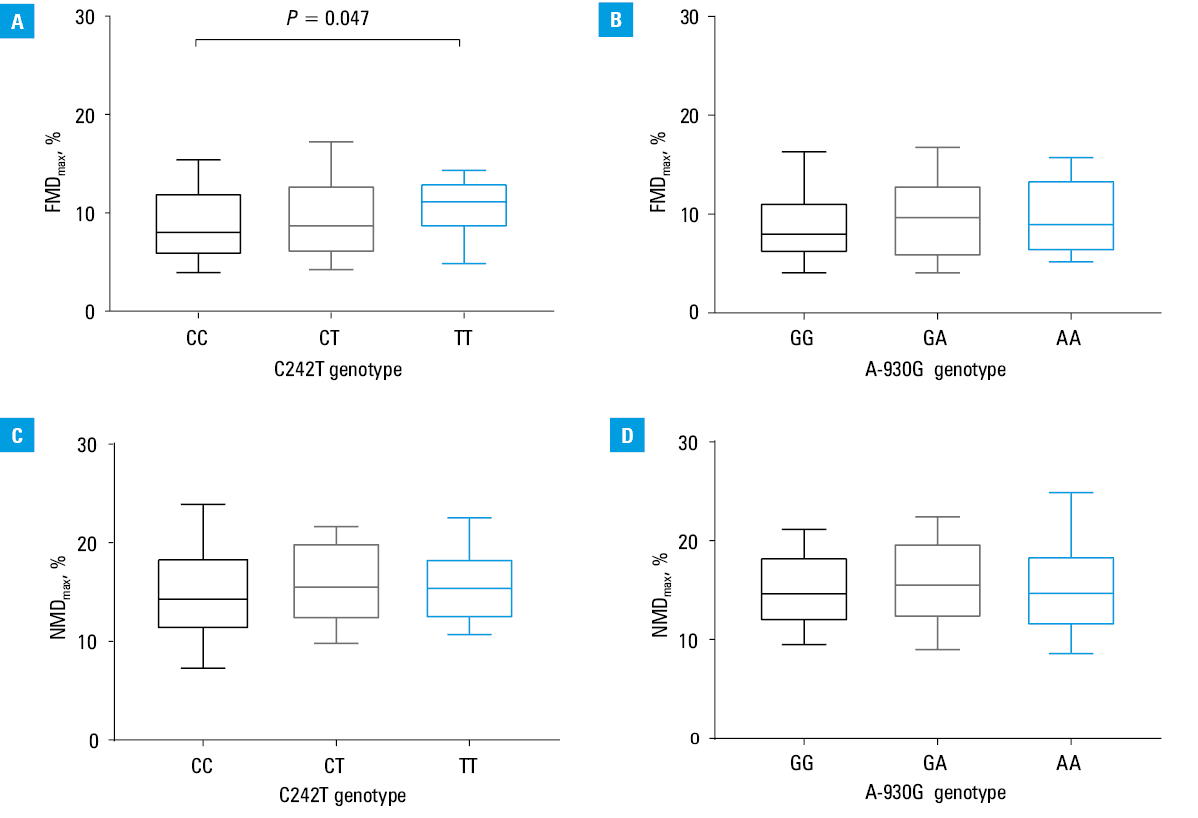
We found no significant differences in mean IMT between the genotypes of both studied polymorphisms (Figure 1A and 1B). We observed a significant association of the C242T polymorphism with maximal FMD in diabetic patients, that is, TT homozygotes were characterized by a significantly elevated FMDmax compared to CC homozygotes (median [interquartile range]: 11.1% [8.5%–13.1%] vs 8% [5.7%–12.1%] respectively; Figure 2A). The observed association was confirmed in a logistic regression model estimating odds for low (below median) FMDmax additionally adjusted for mean IMT (odds ratio [OR] [95% CI], 0.25 [0.08–0.8]; 0.55 [0.33–0.93], and 0.31 [0.11–0.91] for tests involving TT vs CC genotype comparison, additive, and recessive models, respectively). These associations remained robust after additional adjustment for age, current smoking status, or BMI (data not shown). No significant association between the C242T polymorphism and NMD level was observed (Figure 2C). Genotypes of the A‑930G polymorphism were not significantly associated with maximal FMD (Figure 2B). Moreover, no significant association was found when recessive and dominant models of inheritance were tested. Similarly, no significant relationship was found between the genotypes of the A‑930G polymorphism and NMD (Figure 2D). To check whether the CYBA gene polymorphisms correlate with clinical outcome of the disease, we tested their association with ischemic heart disease; however, no significant results were observed (OR [95% CI], 1.42 [0.9–2.23] and 1.2 [0.76–1.9] for an additive [ie, per‑minor allele] model testing the A‑930G and C242T polymorphisms, respectively).
Association between the C242T and A‑930G polymorphisms and drug use or level of biochemical parameters
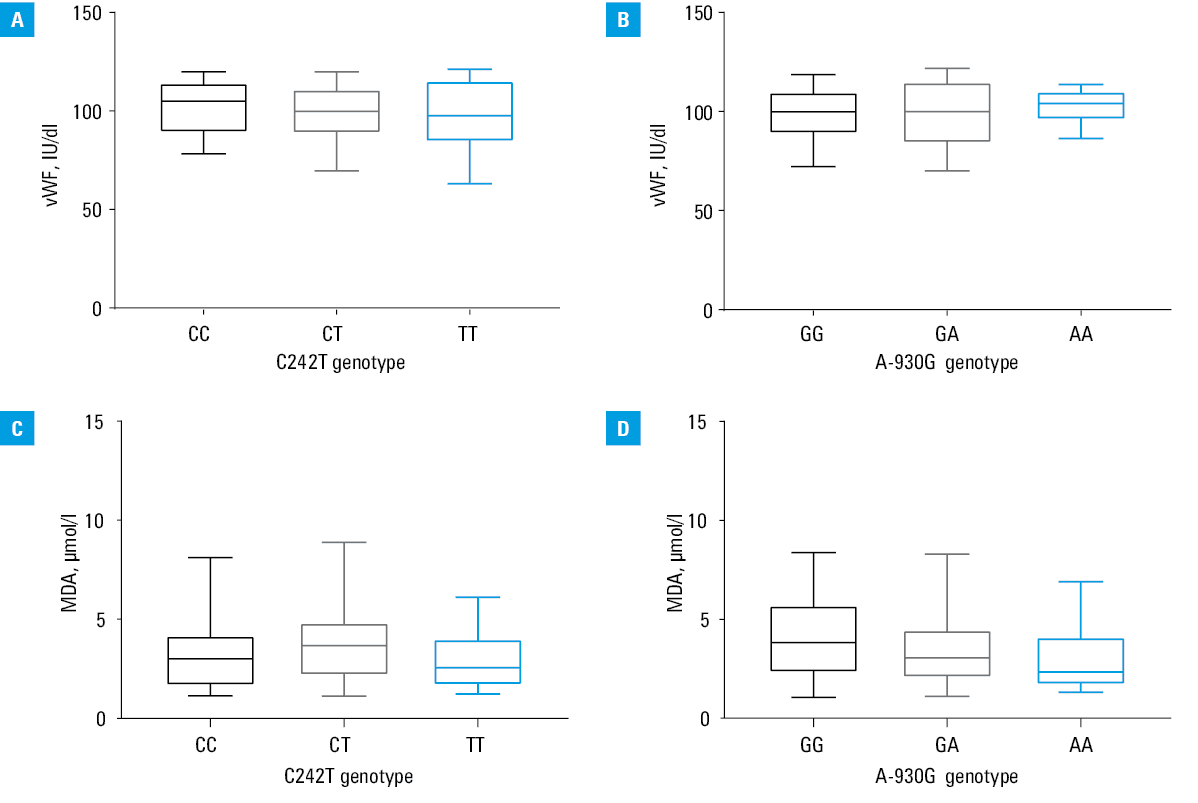
Levels of vWF and MDA (Figure 3A–3D) or biochemical parameters, except for total cholesterol level (Table 2), did not significantly differ between the genotypes studied. We additionally tested whether the C242T and A‑930G polymorphisms were associated with the use of medications reported by patients (Table 1); however, no significant association was found between these SNPs and oral antidiabetic medications, insulin, angiotensin converting enzyme inhibitors, diuretics, statins, acetylsalicylic acid, α- or β-blockers, nitrates, or calcium channel blockers in genotypic, recessive or dominant models in the Pearson’s χ2 test (data not shown).
SNP | C242T | A‑930G | ||||
Genotype | CC | CT | TT | GG | GA | AA |
Data are presented as median (IQR).
a P = 0.03 as compared with the CC/CT genotypes
Abbreviations: CYBA, cytochrome b‑245 alpha chain; SNP, single‑nucleotide polymorphism; others, see Table 1 | ||||||
Total cholesterol, mmol/l | 5.05 (4.47–5.67) | 4.89 (4.33–5.93) | 5.45a (4.95–6.5) | 5.12 (4.63–6.01) | 5.09 (4.44–5.73) | 4.72 (4.33–5.5) |
Triglicerydes, mmol/l | 1.79 (1.27–2.95) | 1.94 (1.44–2.6) | 2.35 (1.56–3.13) | 2.01 (1.33–2.93) | 1.9 (1.34–2.65) | 2 (1.52–2.91) |
LDL cholesterol, mmol/l | 2.88 (2.42–3.44) | 2.87 (2.28–3.63) | 3.08 (2.49–3.92) | 3 (2.55–3.67) | 2.86 (2.26–3.63) | 2.73 (2.3–3.03) |
HDL cholesterol, mmol/l | 1.1 (1–1.34) | 1.13 (0.95–1.29) | 1.24 (0.94–1.43) | 1.1 (0.94–1.33) | 1.18 (1–1.37) | 1.1 (0.93–1.28) |
C‑peptide, mg/ml | 3.31 (1.6–4.44) | 2.9 (1.79–3.74) | 2.82 (1.83–4.04) | 2.99 (2.04–4) | 2.74 (1.59–3.94) | 3.23 (2.08–4.34) |
Creatinine, µmol/l | 78.55 (68.38–94.53) | 75.2 (64.2–87.35) | 70.7 (62.5–81.03) | 76.5 (63.8–93.4) | 75.1 (65.8–87.2) | 75.3 (69.8–84.3) |
HbA1c, % | 7.6 (6.8–8.85) | 7.4 (6.3–8.7) | 7.8 (6.8–8.85) | 7.4 (6.58–8.88) | 7.95 (6.8–9.05) | 7.4 (6–8.1) |
Discussion
The main finding of the current study is the demonstration of a protective effect of the T allele of the C242T CYBA polymorphism on endothelial function in patients with T2DM. This is of importance since, to our knowledge, the association of the CYBA gene polymorphisms and endothelial function has not been tested in diabetic patients so far.
Type 2 diabetes mellitus coexists with and is an important risk factor for cardiovascular diseases that are often characterized by endothelial dysfunction.3,35,36 Activation of NOX enzymes plays an important role in increased ROS production and contributes to the loss of NO bioavailability, endothelial dysfunction, and cardiovascular pathology.8,37 Of interest, elevated activation of NOX has been found in an animal model of 3 comorbidities, including hyperglycemia, which resulted in an impaired endothelial function of coronary arteries as well as left ventricular dysfunction.38 Overall, this implicates a mediating effect of NOX isoforms in the development of vascular dysfunction in T2DM.
Both experimental and clinical studies revealed that endothelial dysfunction is reversible by inhibition of NOX enzymes or by ROS scavengers.39,40 Furthermore, mice lacking the functional p22phox gene are protected against leptin resistance and high‑fat feeding–induced weight gain, while mice overexpressing p22phox develop characteristics of metabolic syndrome.41 Induction of T cell infiltrate into perivascular fat in mice overexpressing p22phox41 additionally points to inflammatory pathways as a link between oxidative stress, obesity, insulin resistance, and diabetes, supported by both human and animal studies.8
Nair et al42 demonstrated decreased maximal FMD and increased IMT values in diabetic patients compared with controls. Impairment of these parameters may precede diabetic vascular complications42 and correlate with the level of NO metabolites in chronic renal failure,43 while FMD negatively correlates with the number of complications in diabetic indviduals.44 The above studies emphasize the need for detailed characterization of both genetic and environmental factors influencing FMD and IMT in patients with T2DM.
Letonja et al45 found that the NADPH C242T polymorphism was not associated with the degree of oxidative stress and carotid atherosclerosis in a group of Slovenian patients with T2DM. On the other hand, Hayaishi‑Okano et al46 demonstrated that T2DM patients with the CT + TT genotype were characterized by significantly lower mean IMT than T2DM patients carrying the CC genotype. Interestingly, no such relationship was observed in controls. Additionally, lower fasting plasma insulin concentration was observed in patients carrying the 242T allele.46 The above data suggest that the effect of the C242T CYBA polymorphism on carotid artery atherosclerosis may depend on the ethnic background of patients with T2DM.
While the T allele of the C242T CYBA polymorphism has been associated with lower odds for metabolic syndrome47 and fatal events related to coronary artery disease48 compared with the C allele, Fan et al49 observed an improved endothelial function in individuals with the CT or TT genotype compared with those carrying the CC genotype in a population‑based sample of young healthy adults. This is in agreement with our results and raises a question about the possible modification of the effect of the C242T SNP in diseased individuals. Of note, Fan et al49 observed an average difference of approximately 0.9% in brachial artery FMD between carriers of the CC and TT genotypes. The effect observed in the current study, that is, a 3% difference in median FMD between both genotypes, might suggest a relatively more pronounced association in T2DM patients compared with the healthy population. The mechanisms which could be involved in the observed FMD improvement include reduced vascular NOX activity (independently of other risk factors for atherosclerosis) and decreased vascular superoxide anion production.8 The 242T allele in CYBA was described as a genetic inhibitor of NOX2 activation in response to high‑glucose in vitro16 and as a predictor of lower risk for recurrence of cardiovascular events in high‑risk patients, and was associated with reduced systemic oxidative stress, determined by plasma levels of 8‑hydroxy‑2’-deoxyguanosine (8‑OHdG).17 In line with these results, functional studies revealed that T allele of the C242T, in contrast to the A‑930G, SNP was associated with lower respiratory burst in neutrophils of healthy subjects and lower phorbol myristate acetate–induced superoxide anion production in peripheral mononuclear cells of hypertensive individuals.18,20 Hypertensive patients also exhibited significantly higher values of vWF than normotensive individuals and this effect was modified by the C242T genotype.18 It is important to note that the endothelium, and particularly eNOS, acts in a paracrine and endocrine manner in various tissues. For example, it mediates the protective effects of nitroglycerin in a cardiac ischemia / reperfusion injury in vivo model.50 Therefore, the genetic predisposition towards increased ROS production and NO inactivation may have broad implications in cardiovascular and immune‑related diseases.
Little is known about the effect of the A‑930G CYBA gene polymorphism on IMT or FMD in healthy or diseased populations. However, it may have functional properties such as that of affecting transcription activity and, ultimately, modulating the gene expression.19 Promoter CYBA variants, particularly the A‑930G polymorphism, have been associated with coronary artery disease in the Polish population.14,15 However, we did not observe a significant association between the A‑930G polymorphism and FMD, IMT, or ischemic heart disease among the investigated patients with T2DM. This suggests that C242T, rather than A‑930G, has functional consequences in diseased individuals, especially those with T2DM. While deep clinical phenotyping of the study patients certainly increased the precision of the genetic effect estimates, a moderate sample size might be perceived as a limitation of our study and could result in a lack of significant association concerning the promoter CYBA polymorphism.
In conclusion, C242T, missense polymorphism of CYBA, significantly correlates with endothelial function in patients with T2DM. Since endothelial function is a genetically complex trait, this polymorphism, among other environmental and genetic factors, may contribute to a risk score for endothelial dysfunction in patients with this disease.
- Egashira K, Hirooka Y, Kai H, et al. Reduction in serum cholesterol with pravastatin improves endothelium‑dependent coronary vasomotion in patients with hypercholesterolemia. Circulation. 1994; 89: 2519‑2524. | Crossref
- Gajos G. Diabetes and cardiovascular disease: from new mechanisms to new therapies. Pol Arch Intern Med. 2018; 128: 178‑186. | Crossref
- Mundi S, Massaro M, Scoditti E, et al. Endothelial permeability, LDL deposition, and cardiovascular risk factors – a review. Cardiovasc Res. 2018; 114: 35‑52. | Crossref
- Konduracka E, Cieślik G, Małecki MT, et al. Obstructive and nonobstructive coronary artery disease in long‑lasting type 1 diabetes: a 7‑year prospective cohort study. Pol Arch Intern Med. 2019; 129: 97‑105. | Crossref
- Haberka M, Machnik G, Kowalówka A, et al. Epicardial, paracardial, and perivascular fat quantity, gene expressions, and serum cytokines in patients with coronary artery disease and diabetes. Pol Arch Intern Med. 2019; 129: 738‑746. | Crossref
ARTICLE INFORMATION