The function of the heart after successful transcatheter mitral valve repair due to severe functional regurgitation
Key words: functional mitral regurgitation, heart strain, transcatheter mitral valve repair



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The function of the heart after successful transcatheter mitral valve repair due to severe functional regurgitation
Introduction: The function of the heart after successful transcatheter edge‑to‑edge mitral valve repair (TMVR) remains not fully investigated.
Objectives: The aim of our study was to assess the direct impact of effective TMVR on the strains of the left atrium (LA), the left ventricle (LV), and the right ventricle (RV) in patients with functional mitral regurgitation due to coronary artery disease or dilated cardiomyopathy.
Patients and methods: Out of a group that successfully underwent TMVR, we selected 28 patients for the analysis. The remodeling of the LA, the LV, and the RV as well as their strains were assessed.
Results: In the short‑term follow‑up, we found a positive change of LA and LV volumes, RV dimensions but not LV ejection fraction. No strain improvement was observed in the pre and post analysis of LV, RV, LA, and LA in phase 3 (contraction phase). We found a deterioration of LA strain in phases 1 (reservoir phase) and 2 (conduit phase) in patients with a history of paroxysmal atrial fibrillation (phase 1, 2.5% [0%–5.47%]; P = 0.01; phase 2, –3.1% [–0.75% to –6.61%]; P = 0.004) and with coronary artery disease (phase 1, 2.2% [–0.82% to 5.47%]; P = 0.049; phase 2, –3.7% [–7.48% to –1.25%]; P = 0.01).
Conclusions: Our data indicate that no improvement of heart strains can be expected after successful TMVR in the short‑term follow‑up, and the function of the LA may even deteriorate in some subpopulations.
What's new?
In this study, we analyzed the critical problem of mechanical and volumetric changes of the left atrium (LA) and both ventricles after successful transcatheter edge‑to‑edge mitral valve repair (TMVR). We included data derived from 3‑dimensional echocardiographic volumetric assessment and speckle‑tracking strain analysis of the LA, the left ventricle (LV), and the right ventricle (RV) obtained before and after a successful TMVR. We found positive volumetric remodeling of the LA and the LV without influence on the LV ejection fraction. The procedures had no positive influence on basic RV parameters. Overall, we did not observe beneficial effects of TMVR on the mechanical strain of the heart. Furthermore, the subgroups of patients with a history of atrial fibrillation and coronary artery disease actually showed deteriorated mechanical strain. The findings from our study need to be considered when implementing medical treatment following TMVR.
Introduction
The interventional repair of functional mitral regurgitation (FMR) is one of the options reserved for patients who are at too high of a risk to undergo cardiac surgery.1 The most commonly used technique is transcatheter mitral valve repair (TMVR), which involves edge‑to‑edge leaflet stitching with a dedicated device (Mitraclip, Abbott or Pascal, Edwards Lifesciences). Although the impact of TMVR was extensively reported in 2 clinical trials, some detailed questions remain unanswered.2-4 The impact of TMVR on heart strains in patients with degenerative valve disease is known.5-7 However, only a few papers refer to larger cohorts of patients with FMR according to the current standardized consensus. Functional mitral regurgitation causes persistent volume overload of the left atrium (LA), which leads to adverse remodeling, dilation, and dysfunction of the LA.8 Hemodynamic changes cause inflammation, myocyte hypertrophy, and interstitial fibrosis of the LA wall.8
Currently, there are 2 modes of echocardiographic functional analysis of the heart. The first is based on a comparison of volume changes during the cardiac cycle (eg, left ventricular [LV] ejection fraction [LVEF]). Routinely, postprocedural LA / LV volume change is used to assess their remodeling and dysfunction. The second and more sophisticated mode is based on the analysis of the deformation of the myocardium by speckle tracking. Summarized information from these 2 methods may provide a better perspective of postprocedural changes in the function of the heart.
Our study presents a holistic approach to the analysis of heart strain after a successful TMVR in patients with severe FMR.
Patients and methods
Endpoints
The primary endpoint was to assess the direct impact of effective TMVR on the strains of the LA, the LV, and the right ventricle (RV) in patients with FMR due to coronary artery disease (CAD) / dilated cardiomyopathy (DCM). The secondary endpoint was to identify potential factors for strain change.
Model
The working model assumed the minimization of all factors other than TMVR that could affect tested parameters (eg, course of the primary disease). We eliminated potential bias, for example from surgical trauma, by including only TMVR patients.
Cohort
We retrospectively reviewed data of 83 consecutive patients referred for TMVR due to mitral regurgitation (MR) at high risk for cardiac surgery. The eligibility criteria were as follows: 1) FMR successfully treated with TMVR (MitraClip) with reduction of effective mitral regurgitant orifice and volume, which changed the grade of MR by 1 class (from severe to moderate), with stenosis not higher than mild. 2) Availability of 2‑dimensional and 3‑dimensional echocardiography images appropriate for all‑segment analysis at baseline and follow‑up (up to 7 days) acquired in patients with optimal perioperative hemodynamic status. 3) Sinus rhythm (SR) at the time of baseline and follow‑up echocardiography. 4) Adequate quality of echocardiographic images including all LA, LV, and RV walls.
We excluded patients with degenerative MR, paced rhythm, chronic atrial fibrillation (AF), cardiac surgery other than coronary artery bypass grafting (CABG), poor image quality, and those with missing or suboptimal images.
We obtained baseline patient demographics and information regarding EuroSCORE II, New York Heart Association class, coronary artery disease (CAD), CABG, prior myocardial infarction (MI), implantation of cardioverter‑defibrillator, history of paroxysmal and persistent AF, chronic obstructive pulmonary disease, and type 2 diabetes mellitus.
For detailed analysis, we divided the cohort into following subgroups: patients without history of AF (SR group), those with history of AF (AF group), those with CAD (CAD group), and those with dilated cardiomyopathy (DCM group).
The details of the TMVR with MitraClip were described previously.9,10
All patients submitted a signed information and consent form, and the study protocol was approved by the review boards of the participating institutions. The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki with its later amendments, and the approval of the Review Board of the Medical University of Warsaw was obtained.
Echocardiography
Clinical characteristics of the cohort are presented in Table 1. Data were acquired on the Philips Epiq 7C/CVXi system (Andover, Massachusetts, United States) equipped with transthoracic S5‑1 or X5‑1 and transesophageal S8‑2t probes. Off‑card analysis was made on the Philips QLAB 13 software with TOMTEC AutoStrain LV/RV/LA application based on speckle tracking. In each patient, the following were measured: 1) LV strain was measured in 3 orthogonal planes on transthoracic echocardiography, that is, apical 4‑chamber, apical 3‑chamber, and apical 2‑chamber planes. Left ventricular global longitudinal strain (LV‑GLS) was calculated automatically. 2) RV global strain (free wall and septum) was measured in the transthoracic apical 4‑chamber view. 3) LA strains were measured in the transthoracic apical 4 chamber view. We measured strains for all 3 LA cycles according to the guidelines8:
Parameter | Value | |
Data are presented as number (percentage) or median (interquartile range).
Abbreviations: AF, atrial fibrillation; CABG, coronary artery bypass graft; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; DCM, dilated cardiomyopathy; ICD, implanted cardioverter‑defibrillator; MI, myocardial infarction; NYHA, New York Heart Association; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide | ||
Male sex | 19 (68) | |
Age, y | 72.5 (67–77) | |
EuroSCORE II | 2.45 (2–3.4) | |
NYHA functional class | II | 12 (43) |
>III | 16 (57) | |
NT‑proBNP, pg/ml | 3260 (1858–6066) | |
History of AF | 20 (7) | |
CAD | 16 (57) | |
DCM | 12 (43) | |
Previous CABG | 8 (29) | |
Previous MI | 14 (50) | |
ICD | 16 (57) | |
COPD | 6 (21) | |
Diabetes | 12 (42) | |
-
Phase 1, or the reservoir phase, begins at the end of ventricular diastole (mitral valve closure) and continues until the mitral valve opening. It encompasses the time of LV isovolumetric contraction, LVEF, and LV isovolumetric relaxation.
-
Phase 2, or conduit phase, lasts from the mitral valve opening through diastasis until the onset of LA contraction in patients in sinus rhythm. In patients with AF, it continues until the end of ventricular diastole (mitral valve closure).
-
Phase 3, or contraction phase, lasts from the onset of LA contraction until the end of ventricular diastole (mitral valve closure) in patients with sinus rhythm.
The QLAB 13 Dynamic Heart Model software (Philips) was used for the volumetric analysis. The full dataset for volumetric analysis was acquired from the apical window. We measured 3‑dimensional LV end‑systolic and end‑diastolic volumes (LV‑ESV and LV‑EDV) and calculated LVEF. From the same acquisition, we calculated the LA volume (LAV) and its index to patient’s body surface area (LAVi). We used the vendor setup for the Dynamic Heart Model. Automatic analyses were supervised by an experienced echocardiographer and corrected when needed (Supplementary material, Figure S1).
Statistical analysis
All data were collected in a dedicated Microsoft Access (365) database. Data were tested for normality using the Shapiro–Wilk test. Continuous variables were expressed as means (SD) or medians (interquartile ranges [IRQs]), as appropriate. Categorical variables were presented as numbers (percentages). Unpaired, continuous variables were compared using the t test or the nonparametric Mann–Whitney test, as appropriate. Paired variables (pre- versus postprocedural) were compared with the Wilcoxon signed‑rank test. Categorical variables were compared using the χ2 or the Fisher exact tests, as appropriate. Intraobserver variability for MR parameters was measured in a sample of 10 random patients using an interclass correlation coefficient. MedCalc for Windows, version 18.11 (MedCalc Software, Ostend, Belgium) was used for the statistical analysis and all reported probability values were 2‑tailed. A P value of less than 0.05 was considered significant.
Results
A total of 28 patients met the eligibility criteria (Tables 1 and 2). The mean (SD) time of follow‑up echocardiography was 2.5 (2–4) days.
Parameter | Pre‑post difference | P value |
Data are presented as median (interquartile range).
Abbreviations: LA, left atrium; LAV, left atrial volume; LAVi, indexed left atrial volume; LVDd, left ventricular end‑diastolic dimension; LV‑EDV, left ventricular end‑diastolic volume; LVEF, left ventricular ejection fraction; LV‑ESV, left ventricular end‑systolic volume; MR‑ERO, mitral regurgitation effective regurgitant orifice; MR‑volume, mitral regurgitation volume; MI, myocardial infarction; MVA, mitral valve area; MV gradient (post), postprocedural mean mitral valve gradient; NA, not applicable; PAF, paroxysmal atrial fibrillation; RV, right ventricle | ||
MR‑ERO, cm2 | 0.2 (0.18–0.26) | <0.001 |
MR‑volume, ml | 25.5 (22–31.3) | <0.001 |
MVA, cm2 | 3.3 (2.9–4) | <0.001 |
MV gradient (post), mm Hg | 3 (2–4) | NA |
LV‑EDV, ml | 12.5 (2.7–17.9) | 0.007 |
LV‑ESV, ml | 14.5 (3–20) | 0.001 |
LVEF, % | 2 (–0.6 to 5.6) | 0.06 |
LVDd, cm | 0.05 (–0.1 to 0.26) | 0.29 |
LAV, ml | 18.5 (5.3–32.8) | <0.001 |
LAVi, ml/m2 | 10.5 (2.4–23.3) | <0.001 |
LA, cm | 0.1 (–0.06 to 0.2) | 0.38 |
RV, cm | 0.2 (–0.06 to 0.3) | 0.04 |
Left ventricular volumes and strain
After the procedure, we observed a significant reduction of LV‑EDV (median [IQR], 12.5 [2.7–17.9] ml; P = 0.007) and LV‑ESV (median [IQR], 14.5 [3–20] ml; P = 0.001).
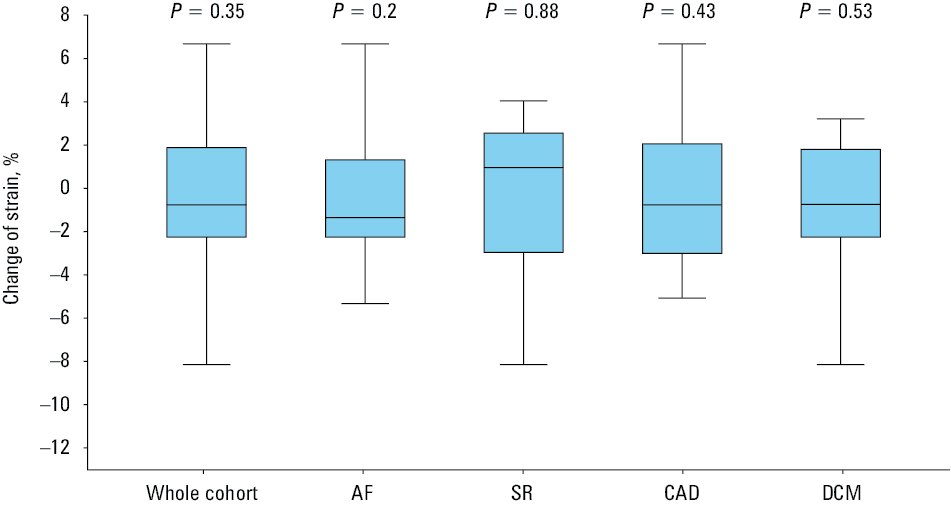
However, there were no significant changes of left ventricular end‑diastolic dimension and LVEF (Table 2). Also, there were no differences in LV‑GLS in pre- and postprocedural assessments in the whole cohort (median [IQR], –0.76% [–2.25% to –0.76%]; P = 0.35) (Figure 1).
Abbreviations: SR, sinus rhythm; others, see Table 1
Right ventricular diastolic dimension and strain
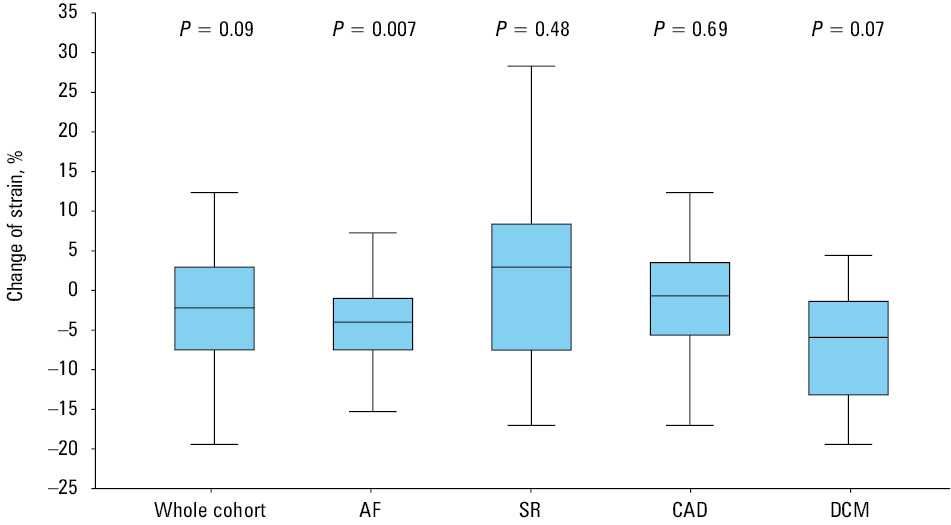
After the procedure, there was a reduction of the right ventricular diastolic dimension (median [IQR], 0.2 [–0.06 to 0.3] cm; P = 0.04) (Table 2). We did not find any differences between RV strain before and after the procedure (median [IQR], –2.2% [–7.52% to 2.92%]; P = 0.09) in the SR, CAD, and DCM groups. However, in the AF group, a deterioration was observed (median [IQR], –4% [–7.52% to –1.04%]; P = 0.007) (Figure 2).
Left atrial volumes and strain
After TMVR, we observed a reduction of LAV (median [IQR], 18.5 [5.3–32.8] ml; P <0.001) and LAVi (median [IQR], 10.5 [2.4–23.3] ml/m2; P <0.001). Pre- and postprocedural dimensions of the LA did not differ.
All phases of LA strain were analyzed separately and globally, including AF, SR, CAD, and DCM groups.
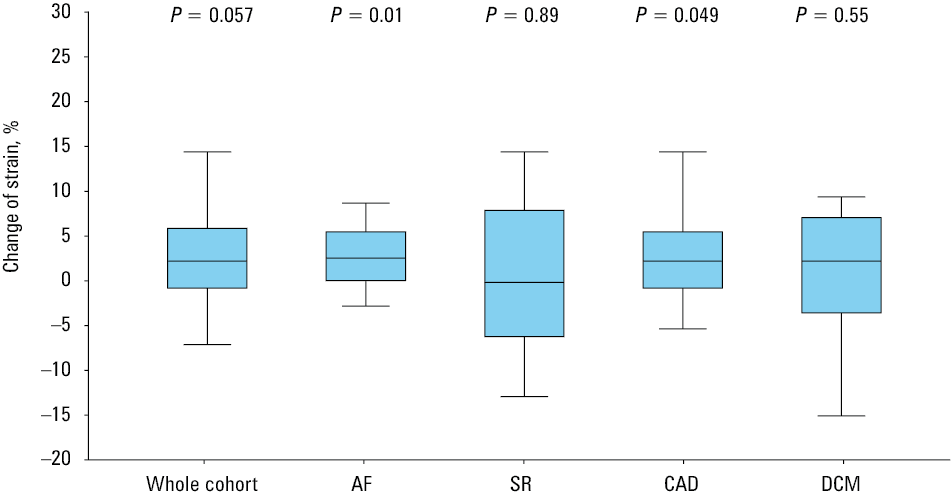
In phase 1, there were no differences between pre- and postprocedural LA strain in the SR and DCM groups (median [IQR], 2.2% [–0.82% to 5.87%]; P = 0.057; Figure 3). However, differences were noted in the AF group (median [IQR], 2.5% [0%–5.47%]; P = 0.01) and the CAD group (median [IQR], 2.2% [–0.82% to 5.47%]; P = 0.049).
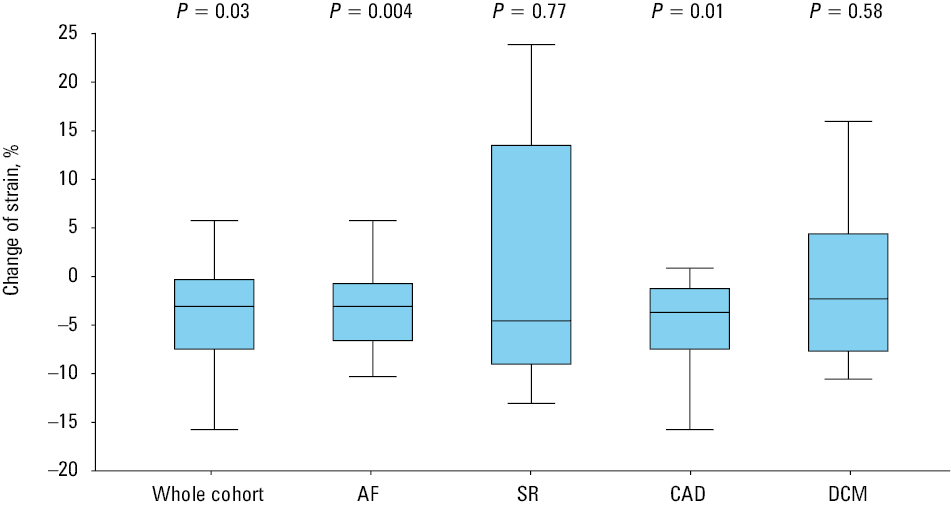
Phase 2 strains differed in global assessment (median [IQR], –3.1% [–0.33% to –7.48%]; P = 0.03). However, this assessment was mainly based on an increase in deteriorating values in the AF group (median [IQR], –3.1% [–0.75% to –6.61%]; P = 0.004) and the CAD group (median [IQR], –3.7% [–7.48% to –1.25%]; P = 0.01) (Figure 4).
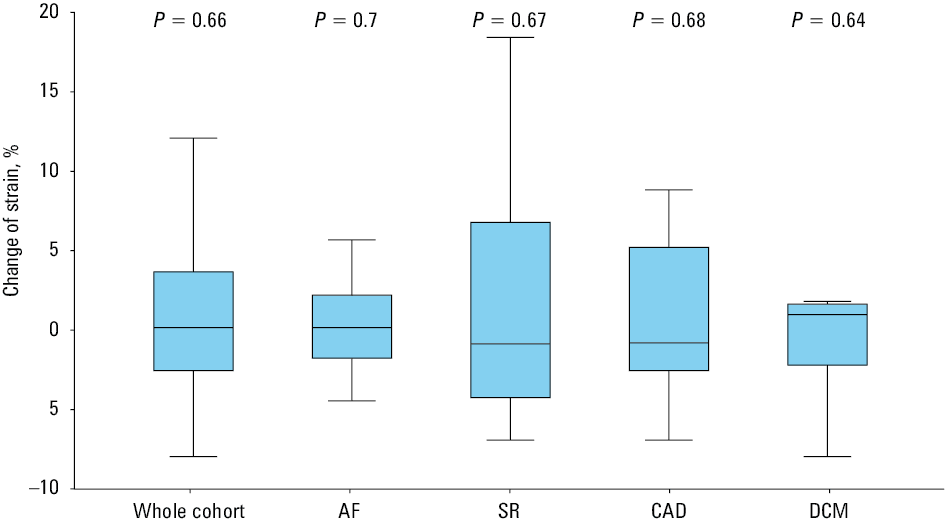
In phase 3, we did not observe any differences in general and subgroup strain assessments in pre- and postprocedural data (median [IQR], –0.14% [–2.58%–3.65%]; P = 0.66) (Figure 5).
Discussion
Numerous studies point to the prognostic value of the heart strain analysis in patients with valve disease at 1‑year follow‑up.11-14 In general, these studies analyzed mixed cohorts of patients not only after transcatheter but also surgical repair. In contrast, our work sheds light on strain fluctuation in the perioperative period after transcatheter repair only. Moreover, we analyzed a cohort of patients with FMR, the assessment of which poses a challenge due to several factors which affect patient clinical and echocardiographic status. In the natural history of CAD or DCM, interstitial fibrosis replaces myocytes. The increase of interstitial fibrosis compromises tissue elasticity and leads to impaired compliance. As a result of a decrease in the amount of myocardiocytes, the contractility of cavities is depressed. Impaired compliance and decreased elasticity of the LA lead to its stiffness—in critical situations of even small volume overload, patients are more susceptible to developing hemodynamic failure, even pulmonary edema.6 This mechanism is universal and we find it both in the tissue of the atria and in the ventricles. In patients with CAD, the process is more localized due to regional ischemia, while in those with DCM, it is more global.
Ventricular parameters
The normalization of LV parameters after valvular procedures depends on numerous factors. Data collected after successful mitral valve surgery due to degenerative regurgitation indicate improvement of LVEF and strains.12
However, our cohort was different. The procedures were introduced in the final stage of heart failure in CAD or DCM. As we anticipated, we observed positive remodeling of the LV: a decrease of LV‑EDV / LV‑ESV after the procedure due to a reduction in primary LV volume overload. As opposed to volume reduction, we did not observe any changes in LVEF, left ventricular end‑diastolic dimension, and LV‑GLS after the procedures. Similarly, we found positive remodeling of the RV but no improvement of its function was detected. These observations are juxtaposed with the results of the COAPT (Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients With Functional Mitral Regurgitation) trial, which suggests that more than 2 weeks are needed for the functional recover of the LV after TMVR. This implies that there should be no rapid change of pharmacotherapy after successful TMVR.3 However, the studied procedures may have been performed too late, in the end stage of the disease, after the point of no return when the interstitial fibrosis was too extensive. Our cohort may be more similar to the population of another large study, the MITRA‑FR (Multicentre Study of Percutaneous Mitral Valve Repair MitraClip Device in Patients With Severe Secondary Mitral Regurgitation) trial, which suggested that this kind of therapy does not improve prognosis.2 The baseline clinical characteristics of our cohort of patients were similar to that of the MITRA‑FR. Our observations could imply that volumetrically significant mitral regurgitation is an effect of remodeling and that the disease is not valvular but myocardial in its origin, and consequently, the reduction of MR did not stop or reverse the primary disease.15-18
Left atrial parameters
Adverse LA remodeling is confirmed in patients with MR.19 It is expected that effective mitral valve disease treatment may result in positive remodeling.20 We observed short‑term reverse LA remodeling (LAV, LAVi) due to preload reduction (postprocedural decrease of MR volume) and left atrial shunt after intra‑atrial septum access.
Based on our observations, positive remodeling is not associated with functional recovery. Moustafa et al21 showed that all phases of atrial strain were depressed in patients with primary chronic MR. Toprak et al22 found an improvement of strains during LA systole and diastole after mitral repair in 1‑year follow‑up. This was substantiated by Ipek et al,6 but only in patients with normal / high LA strain (≥30%) at baseline. Contrary to Toprak et al,22 Ipek et al6 did not observe any improvement of LA strain after TMVR in patients with depressed LA strain (<30%) at baseline.
Our work confirmed these findings and even went a step further. We found that in a group with a history of AF, strain did not improve but deteriorated in phases 1 and 2. Similar findings were noted in the CAD group. However, deterioration was found only during phase 2. In this group of patients, the expected scale of degeneration of the LA wall tissue may even be greater and AF can be treated as a symptom of extensive wall damage.23
From a clinical point of view, the information may be useful to establish perioperative pharmacotherapy when withdrawal of therapy is potentially too aggressive.
Limitations
Due to very restrictive eligibility criteria, we were in a position to only collect data on a small number of patients. However, even studies based on large clinical trials had difficulties in extending the research of similar groups (eg, EVEREST II randomized clinical trial based on 38 such subjects).6,22 We identified 3 main problems in collecting data: 1) for comparative purposes, data should be acquired on the same equipment because sometimes strain analysis is vendor related14; 2) acquiring data on sinus rhythm can be a challenge for end‑stage FMR due to CAD / DCM; and 3) due to implanted cardioverter‑defibrillator / cardiac resynchronization therapy device we could not assess the stage of interstitial fibrosis of the ventricles / LA by cardiac magnetic resonance to support the hypothesis of intervention after the point of no return.
Conclusion
Improvement of the LA, LV, and RV strains cannot be expected in patients with severe FMR with depressed LV function treated with TMVR. Worse still, those with AF and CAD can experience deterioration. However, we observed positive early volumetric remodeling of the LV and the LA, but without influence on LVEF. Our data support the conclusion that in the late stage of FMR with CAD / DCM, TMVR treatment is only a palliative procedure. We believe that current guidelines recommend TMVR too late, when there are no myocytes required for functional recovery, only scar tissue.
- Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017; 38: 2739‑2786. | Crossref
- Obadia JF, Messika‑Zeitoun D, Leurent G, et al. Percutaneous repair or medical treatment for secondary mitral regurgitation. N Engl J Med. 2018; 379: 2297‑2306. | Crossref
- Stone GW, Lindenfeld JA, Abraham WT, et al. Transcatheter mitral‑valve repair in patients with heart failure. N Engl J Med. 2018; 379: 2307‑2318. | Crossref
- Asch FM, Grayburn PA, Siegel RJ, et al. Echocardiographic outcomes after transcatheter leaflet approximation in patients with secondary mitral regurgitation: the COAPT trial. J Am Coll Cardiol. 2019; 74: 2969‑2979. | Crossref
- Öztürk C, Fasell T, Sinning JM, et al. Left atrial global function in chronic heart failure patients with functional mitral regurgitation after MitraClip. Catheter Cardiovasc Interv. 2020; 96: 678‑684. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION