Inflammatory lesions concealing the metastatic process in the course of spondylodiscitis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Inflammatory lesions concealing the metastatic process in the course of spondylodiscitis
Osteoarthritis is a common joint disorder. When affecting the spine, it becomes one of the leading health‑related causes of disability and diminished quality of life.1 Lumbar spine osteoarthritis affects approximately 40% to 85% of the population2; it is the primary differential diagnosis in the case of chronic back pain. At the other end there is spondylodiscitis, which should be taken into consideration in the event of symptom aggravation or current / past history of inflammation. Staphylococcus aureus is the major causative pathogen, and if no clinical improvement is seen after antimicrobial treatment, a follow‑up radiological examination should be performed in search of other possible cause of symptoms.3,4
We present a case of a 66‑year‑old male patient admitted to the emergency department due to exacerbation of recurrent low back pain with lower limb paresis and loss of sensation below the T8 vertebral body lasting for 3 days.
The medical records indicated recent hospitalization (5 months before) in the neurosurgery department due to severe pain in the lumbosacral area and no history of previous trauma. At that time, computed tomography had been performed, revealing lowering of the L1 to L4 vertebral body height with L4 body destruction and a cystic lesion adjacent bilaterally to the iliac arteries. For this reason, contrast‑enhanced magnetic resonance imaging (MRI) had also been carried out. It confirmed vertebral destruction and collection of inflammatory fluid (Figure 1A–1C). Laboratory tests had showed elevated concentrations of C‑reactive protein (135 mg/l; reference range <5 mg/l) and normal procalcitonin levels (0.18 ng/ml). The pus culture had been negative for aerobes, anaerobes, and tuberculosis. The patient had undergone abscess drainage and received antibiotics (ciprofloxacin and rifampicin). His medical history was also positive for alcohol withdrawal syndrome and recent‑onset arterial thrombosis of the lower extremities with subacute ischemia of the left lower limb.
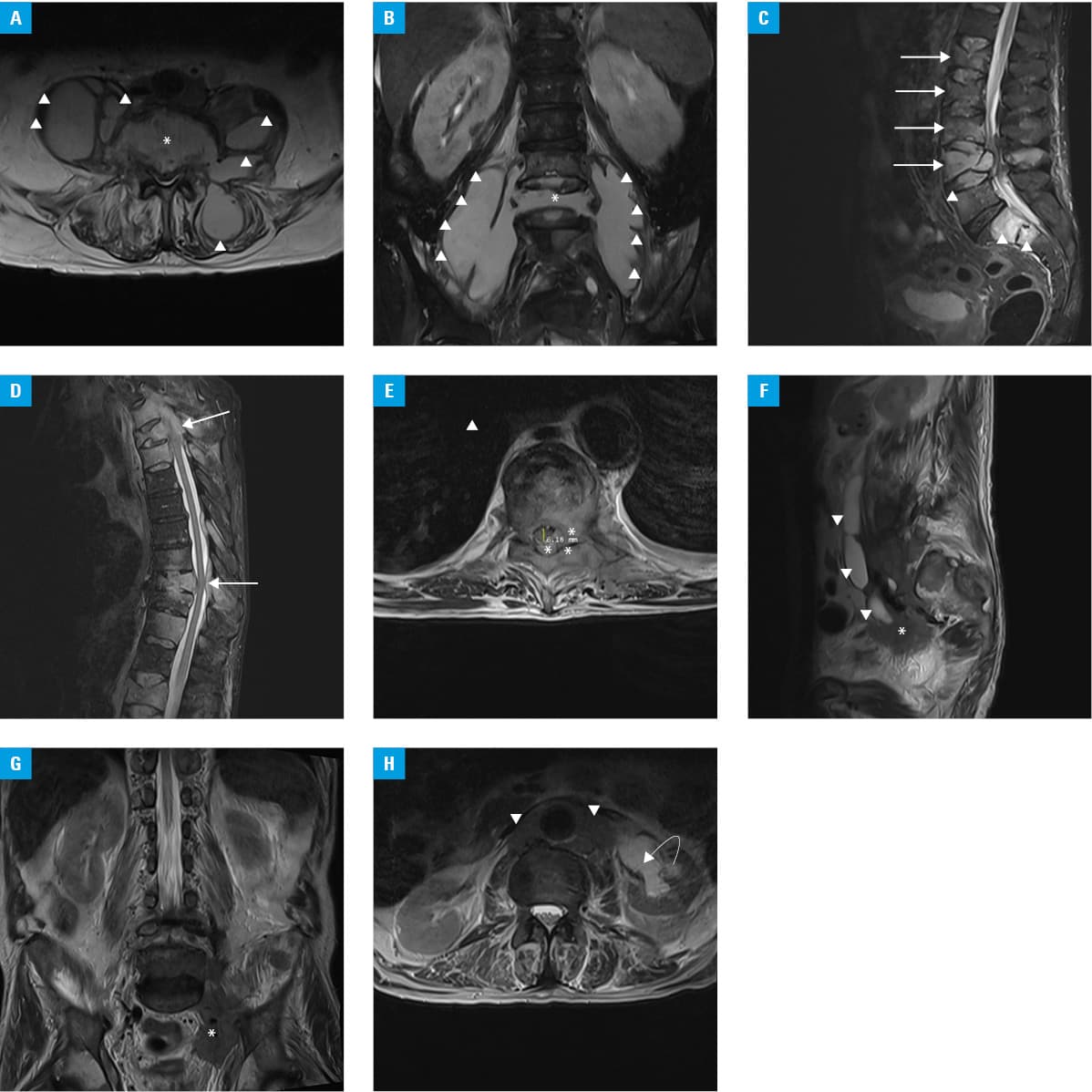
Such extensive medical history prompted a decision to perform both computed tomography and contrast‑enhanced MRI of the spine, which showed complete regression of the purulent lesions within the paravertebral and dorsal muscles. However, progression of the para‑aortic pathological infiltration was observed. Pathological areas were found bilaterally within the sacroiliac joints and ilia. Low signal of the prostate on T2‑weighted MRI images was seen, raising the suspicion of disseminated malignancy that was previously concealed by inflammatory lesions. Such scenario could also explain multiple T1 and T2 hypointense lesions of the thoracic vertebrae with pathological contrast enhancement—most probably consistent with metastases causing spinal stenosis, spinal cord compression, and edema at the T3 and T9 levels (Figure 1D–1H).
The level of prostate‑specific antigen was found to be elevated; biopsy revealed prostate cancer with a Gleason score of 8. The patient received anti‑inflammatory and pain‑relief medications, and was referred to the oncology department to continue the treatment.
The spine is the most common (90%) localization of prostate cancer metastases, especially its lumbar (97%) and thoracic sections.5 The presented clinical case clearly indicates that robust inflammatory infiltrations of the spine and paravertebral soft tissues may obscure metastatic lesions. It seems legitimate to perform further work‑up (contrast‑enhanced MRI or biopsy, if required) and evaluate the primary diagnosis if no clinical improvement is observed after targeted treatment for spondylodiscitis.
- Lindsey T, Dydyk AM. Spinal osteoarthritis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. https://www.ncbi.nlm.nih.gov/books/NBK553190/. Accessed May 4, 2021.
- Goode AP, Carey TS, Jordan JM. Low back pain and lumbar spine osteoarthritis: how are they related? Curr Rheumatol Rep. 2013; 15: 305. | Crossref
- Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010; 65:11‑24. | Crossref
- Bubendorf L, Schöpfer A, Wagner U, et al. Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum Pathol. 2000; 31: 578‑583. | Crossref
- Lee C, Lee S, Bae J. Contiguous spinal metastasis mimicking infectious spondylodiscitis. J Korean Soc Radiol. 2015; 73: 408‑412. | Crossref
ARTICLE INFORMATION