Three-year mortality after acute myocardial infarction in patients with different diabetic status
Key words: diabetes mellitus, hyperglycemia, myocardial infarction, new-onset diabetes mellitus, Polish Registry of Acute Coronary Syndromes (PL-ACS)



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Three-year mortality after acute myocardial infarction in patients with different diabetic status
Introduction: The prevalence of diabetes mellitus (DM) in patients with myocardial infarction (MI) is estimated at about 25%. Short- and long‑term prognosis is worse in patients with DM and hyperglycemia compared with nondiabetics.
Objectives: Our aim was to analyze the impact of DM and transient hyperglycemia on in‑hospital complications and long‑term outcomes in patients with MI.
Patients and methods: We evaluated a prospective cohort of 58 394 patients with MI in the Polish Registry of Acute Coronary Syndromes (PL‑ACS) in terms of in‑hospital complications and 30‑day, 12‑month, and 36‑month outcomes between 2009 and 2012.
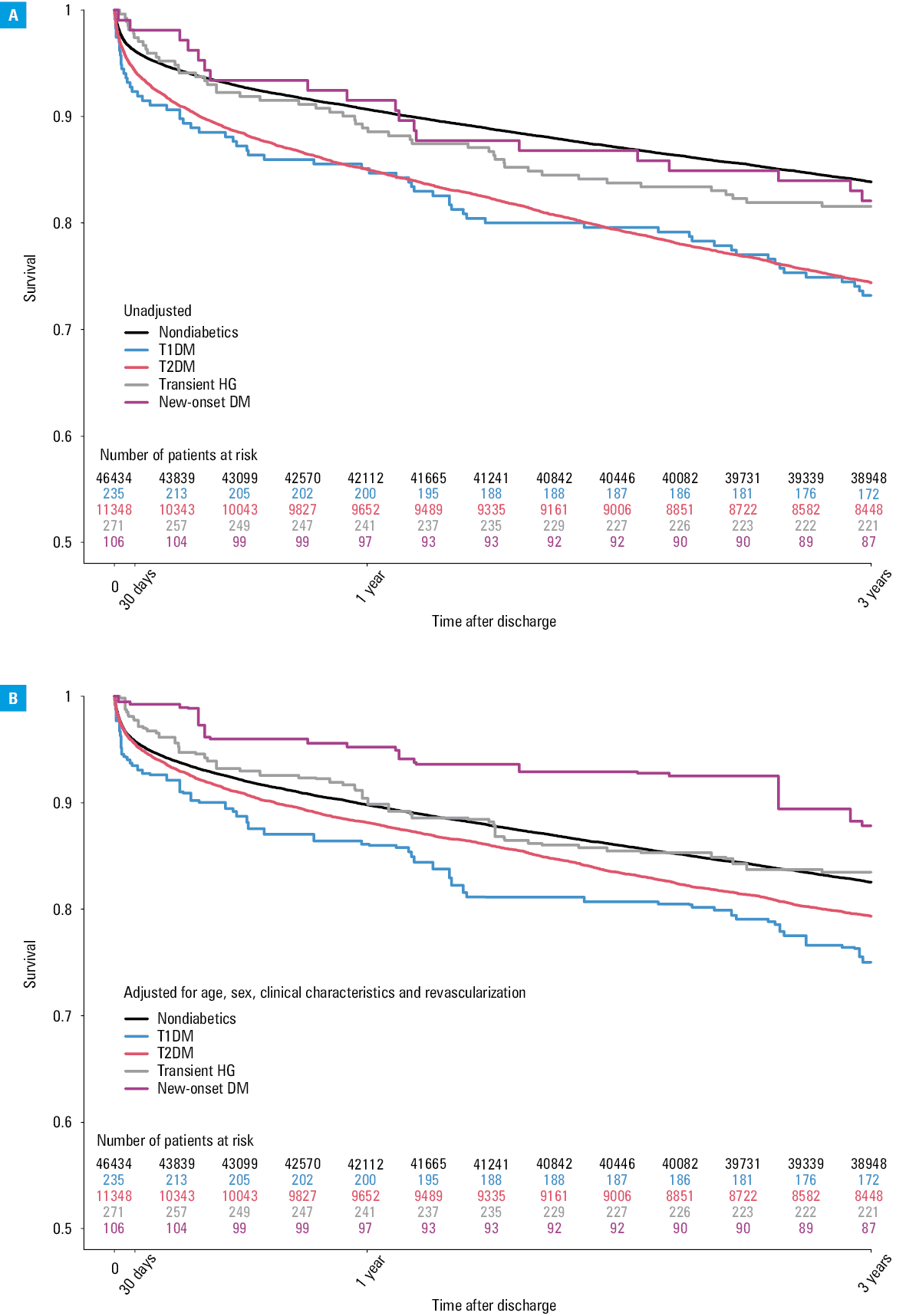
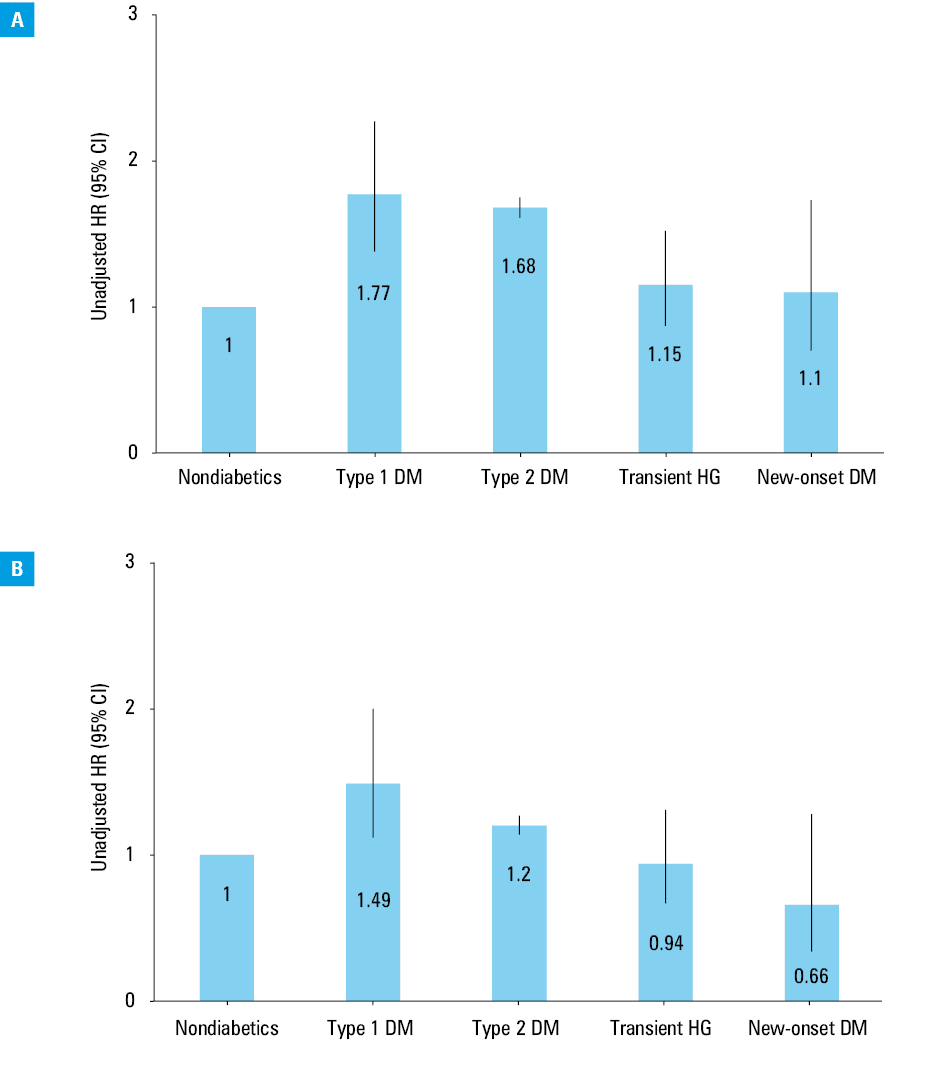
Results: Patients with type 1 DM (T1DM) and type 2 DM (T2DM) underwent invasive diagnostic and therapeutic procedures less frequently than those without diabetes, transient hyperglycemia, and new‑onset DM (P <0.001). T2DM was associated with a significantly higher risk of MI complicated by cardiogenic shock. The rates of pulmonary edema in the transient hyperglycemia group and the DM group were 2‑fold higher than in the nondiabetic group (P <0.001). T1DM and T2DM were associated with a significantly higher risk of death. Unadjusted 3‑year all‑cause death rates in patients with T1DM, T2DM, transient hyperglycemia, new‑onset diabetes and those without diabetes were 26.8%, 25.6%, 18.5%, 17.9%, and 16.2%, respectively. Hazard ratios (95% CI) adjusted for age, sex, clinical characteristics, and revascularization were 1.49 (1.12–2.00), 1.20 (1.14–1.27), 0.94 (0.67–1.31), and 0.66 (0.34–1.28), respectively.
Conclusions: T1DM and T2DM are associated with elevated in‑hospital and long‑term mortality rates after MI. Diabetics and patients with transient hyperglycemia are more likely to develop significant in‑hospital complications compared with nondiabetics. No significant differences regarding acute mechanical complications were noted between populations.
What's new?
Patients with myocardial infarction (MI) and previously diagnosed diabetes mellitus (DM), new‑onset DM, and transient hyperglycemia have a worse prognosis compared with their nondiabetic counterparts. However, many studies concerning treatment results were conducted during the thrombolytic era. Relatively little is known about the outcomes of patients with elevated glucose levels during hospitalization without previous DM diagnosis or patients with new‑onset DM. We therefore included 2 additional classifications in our study for patients with acute MI in regard to glycemic status during hospitalization. We evaluated a nationwide prospective cohort of over 58 000 patients with MI in terms of in‑hospital complications and long‑term outcomes over a 3‑year period per different carbohydrate disorder type: type 1 DM, type 2 DM, new‑onset DM, and transient hyperglycemia. In contrast with previous publications, this study is not limited to admission glucose levels only but includes blood glucose monitoring throughout hospitalization.
Introduction
The prevalence of diabetes mellitus (DM) in patients with acute coronary syndrome (ACS) is estimated at about 25%, and the prognosis is worse compared with that of nondiabetic patients.1,2 Moreover, DM proved to be a risk factor for complications of myocardial infarction (MI) and increased mortality.3-6 It is also associated with an elevated risk of early MI complications, such as cardiogenic shock and heart failure (HF), as diabetic patients exhibit limited left ventricular remodeling after MI.7,8 Controversy remains regarding the prevalence of transient hyperglycemia in nondiabetic patients hospitalized with MI and its impact on outcomes and long‑term mortality. In some cases, elevated blood glucose levels will result in a diagnosis of new‑onset DM, whereas in other cases, hyperglycemia is transient and may be associated with a stress response,9 resulting from the secretion of steroid hormones, adrenaline, glucagon, and the release of free fatty acids.10 Nondiabetic patients with an increased fasting glycemia on admission to the hospital due to ACS are at a significantly increased risk for developing DM and at a greater long‑term mortality risk.11,12 Among nondiabetic patients hospitalized with ACS, a fasting hyperglycemia of at least 180 mg/dl (10 mmol/l) predicted 1‑year mortality and was associated with a 4‑fold increased risk of DM at 1 year.11 This finding is also stressed in a study by Ritsinger et al12 in which the authors suggest that prophylactic treatment for increased blood glucose levels should be initiated before discharge from the coronary care unit. In accordance with aforementioned conclusions from previous studies, our analysis concentrated on both in‑hospital outcomes and all‑cause death rates assessed incrementally at 4 different time points. Our study aimed to compare a control group of patients with MI but without diabetes with a group of patients with MI and DM or transient hyperglycemia (stratified into type 1 DM [T1DM], type 2 DM [T2DM], new‑onset DM, and transient hyperglycemia groups) in terms of patient characteristics, treatment, and in‑hospital, 30‑day, 12‑month, and 36‑month outcomes.
Patients and methods
Data for this analysis were collected from the Polish Registry of Acute Coronary Syndromes (PL‑ACS), a nationwide, multicenter, prospective registry of consecutively hospitalized patients with ACS in Poland. The registry includes data of 58 394 consecutive patients admitted to Polish hospitals from 2009 to 2012. The PL‑ACS registry is a joint initiative of the Silesian Center for Heart Diseases in Zabrze and the Polish Ministry of Health. Logistic support is provided by the Polish National Health Fund (Narodowy Fundusz Zdrowia [NFZ]). The design of the PL‑ACS has been described previously.13 The number of people hospitalized due to acute myocardial infarction (AMI) fluctuated within the limits of 77 200 in 2009 to 79 400 in 2012. Our data account for approximately 25% of all MIs in Poland and were collected in hospitals with an invasive cardiology laboratory and community hospitals without percutaneous coronary intervention (PCI) facilities.
The registry includes data on demographics, medical history, treatment, and post‑MI in‑hospital complications. Additionally, follow‑up data were obtained from the NFZ. The follow‑up data at 30 days, 12 months, and 36 months after MI‑related hospitalization were available for all enrolled patients.
For the purposes of our current study, only data of patients with MI were analyzed. The definitions for the initial diagnosis of ST‑segment elevation MI (STEMI) and non‑STEMI (NSTEMI) were as follows:
-
STEMI was defined as the presence of 1) typical angina and / or symptoms of ischemia at rest lasting more than 20 minutes, 2) electrocardiography abnormalities consistent with MI (ST‑segment elevation of 2 mm in adjacent chest leads and / or ST‑segment elevation of 1 mm in 2 standard leads or new left bundle branch block, and 3) positive markers of myocardial necrosis.
-
NSTEMI was defined as the presence of 1) typical angina and / or symptoms of ischemia at rest lasting more than 20 minutes, 2) the absence of ST‑segment elevation as defined earlier, and 3) positive markers of myocardial necrosis.
Study patients were divided into 5 groups: patients with T1DM, T2DM, transient hyperglycemia, new‑onset DM, and a control group of nondiabetics.
The diagnosis of DM was determined based on patients’ records (documented DM treated with insulin, oral hypoglycemic drugs, or diet). New‑onset DM was diagnosed based on at least 2 instances of fasting plasma glucose levels of more than 125 mg/dl (7.0 mmol/l) after AMI, a random plasma glucose level of more than 200 mg/dl (11.1 mmol/l), or blood glucose levels of more than 200 mg/dl (11.1 mmol/l) as determined by a 2‑hour oral glucose tolerance test performed at the end of hospitalization. Transient hyperglycemia was diagnosed when the patient required administration of short‑acting insulin via an infusion or subcutaneous injection during the treatment for MI, but new‑onset diabetes was excluded by the end of hospitalization. The patients who were diagnosed with DM during hospitalization following the acute phase of MI, but their daily demand for insulin was under 30 units, were prescribed oral hypoglycemic agents or an appropriate diet; otherwise, intensive insulin therapy was continued.
In‑hospital and long‑term complications were defined as follows:
-
Death: death due to all causes.
-
Reinfarction: an ischemic event meeting the European Society of Cardiology / American College of Cardiology criteria for MI which was clearly clinically distinct from the index event on admission.
-
Stroke (hemorrhagic or ischemic): an acute neurologic deficit lasting more than 24 hours and affecting the ability to perform daily activities or resulting in death.
-
Major bleeding: overt clinical bleeding that 1) was associated with a decrease in hemoglobin levels of more than 50 g/l (5 g/dl) or an absolute decrease in hematocrit levels of more than 15%, or 2) caused hemodynamic compromise, or 3) required blood transfusion.
-
Cardiogenic shock: hypotension (systolic blood pressure of <90 mm Hg for at least 30 minutes or the need for inotropes or vasopressors or intra‑aortic balloon pump counterpulsation to maintain a systolic blood pressure of >90 mm Hg) and hypoperfusion (cool extremities or a urine output of <30 ml/h, and a heart rate of ≥60 bpm).
An invasive procedure was defined as coronary angiography during index hospitalization. PCI was defined as a coronary intervention, such as plain old balloon angioplasty or stent implantation.
We also compared the study groups in terms of clinical presentation, patient characteristics, and cardiovascular risk factors. Differences in treatment strategies, including angiography, PCI, and coronary artery bypass grafting (CABG) were also scrutinized. Our analyses additionally included in‑hospital complications of MI. Outcome data were collected at 4 different time points: during hospital stay, as well as during follow‑up at 30 days, 1 year, and 3 years. We performed an analysis for 3‑year all‑cause death adjusted for age, sex, clinical characteristics, and revascularization.
Statistical analysis
Continuous variables were presented as means (SD). Categorical variables were presented as percentages and numbers. For the in‑hospital data analysis, we used the χ2 test for qualitative data and analysis of variance for continuous data to test the differences between the groups. The unadjusted and adjusted hazard ratios were calculated for selected variables in the study groups versus the control group with the use of the Cox proportional hazards regression model. The association between the groups and long‑term all‑cause death were analyzed using the unadjusted and adjusted Kaplan–Meier method for multiple‑group comparisons. Adjusted survival and hazard ratios were calculated using the inverse probability method. A P value of less than 0.05 was considered statistically significant. All reported P values are 2‑tailed. Analyses were performed with the use of Statistica, version 13 (TIBCO Software Inc, 2017, Palo Alto, California, United States), 2020 NCSS Statistical Software (NCSS LLC, Kaysville, Utah, United States), and R, version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics
The investigation conformed to the principles outlined in the Declaration of Helsinki and was carried out in accordance with the local ethics committee’s policy. The study was not a medical experiment and therefore did not require approval by a local ethics committee. The Ethics Committee of the Medical University of Warsaw in Poland was informed about the study (AKBE/81/2019) on March 11, 2019. Written informed consent was not required.
Results
Between January 2009 and December 2012, out of 58 394 patients who presented with MI, 11 348 (19.4%) had T2DM, 235 (0.4%) had T1DM, 271 (0.5%) had transient hyperglycemia, and 106 (0.2%) had new‑onset diabetes. Women accounted for 35.2% of the entire study cohort. Table 1 shows the baseline characteristics of all patients with MI stratified by their respective diabetic status. Compared with nondiabetic patients, those with T2DM or transient hyperglycemia were, on average, older. Patients with transient hyperglycemia or DM were more likely to have a higher body mass index than those without DM and were more likely to have hyperlipidemia as well as hypertension. Patients with T1DM and T2DM were more likely to be former smokers while those without DM were more likely to be current smokers. The lowest proportions of patients with a history of coronary artery disease (CAD), MI, CABG, HF, and stroke were found in the nondiabetic group.
Parameter | Nondiabetics (n = 46 434) | T1DM (n = 235) | T2DM (n = 11 348) | Transient HG (n = 271) | New‑onset DM (n = 106) | P valuea | |
Data are presented as percentage, unless otherwise indicated.
a the χ2 independence test
b BMI was calculated as the weight in kilograms divided by the square of the height in meters.
Abbreviation: BMI, body mass index; CABG, coronary artery bypass grafting; CVD, cardiovascular disease; DM, diabetes mellitus; HF, heart failure; HG, hyperglycemia; MI, myocardial infarction; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus | |||||||
Male sex | 67.2 | 60.0 | 55.2 | 57.2 | 57.6 | <0.001 | |
Age, y, mean (SD) | 64.4 (12.1) | 63.2 (13.0) | 68.6 (10.3) | 67.3 (11.0) | 64.1 (10.6) | <0.001 | |
BMIb, kg/m2, mean (SD) | 27.2 (4.3) | 28.4 (5.4) | 29.7 (5.1) | 30.1 (5.2) | 30.0 (4.6) | <0.001 | |
Hypertension | 68.4 | 77.0 | 85.0 | 77.9 | 82.1 | <0.001 | |
Hyperlipidemia | 41.0 | 44.7 | 48.0 | 48.0 | 55.7 | <0.001 | |
Smoking status | Former smoker | 27.4 | 37.9 | 34.1 | 21.4 | 22.6 | <0.001 |
Current smoker | 34.6 | 20.4 | 17.4 | 27.3 | 22.6 | <0.001 | |
Chronic kidney disease | 4.3 | 15.7 | 11.2 | 5.5 | 6.6 | <0.001 | |
History | |||||||
CVD in the family | 11.4 | 15.7 | 12.8 | 12.2 | 9.4 | <0.001 | |
Coronary artery disease | 10.8 | 21.7 | 21.3 | 14.0 | 17.0 | <0.001 | |
MI | 12.6 | 18.7 | 20.0 | 14.0 | 17.0 | <0.001 | |
PCI | 7.5 | 10.2 | 12.1 | 7.8 | 12.3 | <0.001 | |
CABG | 2.2 | 3.8 | 4.2 | 1.1 | 1.9 | <0.001 | |
HF | 6.2 | 10.6 | 10.8 | 8.5 | 13.2 | <0.001 | |
PAD | 4.0 | 7.2 | 6.3 | 5.5 | 2.8 | <0.001 | |
Stroke | 3.2 | 5.1 | 6.0 | 4.1 | 5.7 | <0.001 | |
Invasive procedures (coronary angiography) were used in more than 90% of patients in all 5 groups, although various treatment strategies were used during hospitalization. Fewer patients with T1DM and T2DM underwent invasive diagnostic or therapeutic procedures compared with patients with transient hyperglycemia, new‑onset DM, and nondiabetics (P <0.001) (Table 2).
Procedure | Nondiabetics (n = 46 434) | T1DM (n = 235) | T2DM (n = 11 348) | Transient HG (n = 271) | New‑onset DM (n = 106) | P valuea |
Data are presented as number (percentage).
a the χ2 independence test
Abbreviation: see Table 1 | ||||||
Cardiac catheterization | 43 781 (94.3) | 212 (90.2) | 10 375 (91.4) | 262 (96.7) | 103 (97.2) | <0.001 |
PCI | 36 979 (79.6) | 166 (70.6) | 8464 (74.6) | 238 (87.8) | 92 (86.8) | <0.001 |
CABG | 1236 (2.7) | 8 (3.4) | 371 (3.3) | 1 (0.4) | 1 (0.9) | <0.001 |
The diagnosis of multivessel disease (MVD) was more common in T1DM, T2DM, and transient hyperglycemia groups (65.6%, 60.7%, and 59.5%, respectively) than in the control group (53.33%; P <0.001). The lowest rates of PCI were observed in patients with T1DM (70.6%) and T2DM (74.6%). CABG surgery was more frequent in both T1DM and T2DM (3.4% and 3.3%, respectively) in contrast to the new‑onset diabetes, transient hyperglycemia, and control groups (0.9%, 0.4%, and 2.7%, respectively; P <0.001).
In‑hospital post‑MI complications stratified by the patients’ diabetes status are presented in Table 3. There were differences between the study groups in the risk of the following complications: cardiogenic shock (P <0.001), pulmonary edema (P <0.001), in‑hospital cardiac arrest (P = 0.004), bleeding (P = 0.006), stroke (P = 0.48), the need of pacemaker implantation (P = 0.002), and death (P <0.001). We recorded a reinfarction rate of up to 1.3% in patients in the DM groups (vs 0.3% in nondiabetics) during hospitalization (P = 0.05).
In‑hospital complications | Nondiabetics (n = 46 434) | T1DM (n = 235) | T2DM (n = 11 348) | Transient HG (n = 271) | New‑onset DM (n = 106) | P valuea |
Data are presented as number (percentage).
a the χ2 independence test
Abbreviations: CRT‑D, cardiac resynchronization therapy‑defibrillator; ICD, implantable cardioverter‑defibrillator; MR, mitral regurgitation; others; see Table 1 | ||||||
Cardiogenic shock | 586 (1.3) | 3 (1.3) | 205 (1.8) | 5 (1.9) | 0 | <0.001 |
Free‑wall rupture | 35 (0.1) | 0 | 8 (0.1) | 0 | 0 | 0.97 |
Ventricular septal rupture | 30 (0.1) | 0 | 8 (0.1) | 0 | 0 | 0.98 |
Acute MR | 19 (0.0) | 0 | 13 (0.1) | 0 | 0 | 0.05 |
Pulmonary edema | 482 (1.0) | 5 (2.1) | 226 (2.0) | 6 (2.2) | 2 (1.9) | <0.001 |
Reinfarction | 131 (0.3) | 3 (1.3) | 40 (0.4) | 1 (0.4) | 0 | 0.05 |
In‑hospital cardiac arrest | 981 (2.1) | 8 (3.4) | 299 (2.6) | 3 (1.1) | 1 (0.9) | 0.004 |
Bleeding | 668 (1.4) | 5 (2.1) | 200 (1.8) | 9 (3.3) | 0 | 0.006 |
Stroke | 103 (0.2) | 1 (0.4) | 43 (0.4) | 1 (0.4) | 0 | 0.048 |
Pacemaker | 193 (0.4) | 1 (0.4) | 78 (0.7) | 3 (1.1) | 0 | 0.002 |
ICD / CRT‑D | 96 (0.2) | 0 | 23 (0.2) | 0 | 1 (0.9) | 0.42 |
All‑cause death | 1527 (3.3) | 14 (6.0) | 549 (4.8) | 0 | 1 (0.9) | <0.001 |
T2DM was associated with a significantly higher relative risk (RR) of MI complicated by cardiogenic shock (RR, 1.43; 95% CI, 1.22–1.68). The RR of cardiogenic shock for the transient hyperglycemia group was greater than 1 (RR, 1.46; 95% CI, 0.61–3.50), but the CI contained the null value. A larger study group would be required for a narrower CI. The RR of cardiogenic shock in T1DM was 1.01 (95% CI, 0.33–3.12), and for new‑onset DM, it was 0.37 (95% CI, 0.02–5.88).
Pulmonary edema was approximately 2‑fold more common in the transient hyperglycemia and DM groups than in the nondiabetic group (1.9%–2.1% vs 1.0%; P <0.001). Patients with T1DM had the highest rates of cardiac arrest during hospitalization. In‑hospital all‑cause mortality was the highest in the T1DM and T2DM groups (6% and 4.8%, respectively). There were no differences between the transient hyperglycemia or DM groups and the control group regarding acute mechanical complications, such as free‑wall rupture, ventricular septum rupture, or acute mitral regurgitation. However, the differences with regard to acute mitral regurgitation and reinfarction tended to be significant (P = 0.05). Bleeding complications were more frequent in the T2DM group compared with the control group (1.8% vs 1.4%; P = 0.01) and in the transient hyperglycemia group compared with the control group (3.3% vs 1.4%; P = 0.01). There were no differences between the T1DM or new‑onset diabetes groups and the control group.
The in‑hospital, 30‑day, 12‑month, and 36‑month outcomes are presented in Table 4. The 3‑year all‑cause death rates in patients with T1DM, T2DM, transient hyperglycemia, new‑onset diabetes, and the control group were 26.8%, 25.6%, 18.5%, 17.9%, and 16.2%, respectively (P <0.001). The lowest long‑term survival was in the T1DM and T2DM groups. Three‑year survival in the study groups is presented in Figure 1A and 1B. After adjustment for age, sex, clinical characteristics, and revascularization, patients with T1DM had the worst 3‑year survival, followed by those with T2DM. Consequently, T1DM and T2DM were associated with a significantly higher RR of 3‑year all‑cause death both in unadjusted (RR, 1.77; CI 95%, 1.38–2.27 and RR, 1.68; CI 95%, 1.61–1.75, respectively) and adjusted analyses (Figure 2A and 2B and Supplementary material, Figures S1 and S2 and Table S1).
Follow‑up | Nondiabetics (n = 46 434) | T1DM (n = 235) | T2DM (n = 11 348) | Transient HG (n = 271) | New‑onset DM (n = 106) | P valuea |
Data are presented as number (percentage).
a the χ2 independence test
Abbreviations: see Table 1 | ||||||
In‑hospital | 1527 (3.3) | 14 (6.0) | 4.8 (549) | 0 | 0.9 (1) | <0.001 |
30‑day (including hospitalization) | 1795 (3.9) | 18 (7.7) | 655 (5.8) | 7 (2.6) | 2 (1.9) | <0.001 |
12‑month | 4325 (9.3) | 35 (14.9) | 1699 (15.0) | 30 (11.1) | 9 (8.5) | <0.001 |
36‑month | 7502 (16.2) | 63 (26.8) | 2910 (25.6) | 50 (18.5) | 19 (17.9) | <0.001 |
Abbreviations: see Table 1
Abbreviations: see Table 1
Discussion
Our large, nationally representative study of patients hospitalized with AMI showed that the risk of in‑hospital complications and long‑term mortality is contingent upon respective diabetic status. Our principal findings include: 1) lower frequency of invasive diagnostic or therapeutic procedures in patients with DM; 2) significant in‑hospital complications in diabetic and transient hyperglycemic patients; 3) significantly higher RR of MI complicated by cardiogenic shock in patients with T2DM; 4) twice as high rates of pulmonary edema in the transient hyperglycemia and DM groups compared with the nondiabetic group; 5) no differences between groups in terms of acute mechanical complications; 6) the highest overall in‑hospital and 3‑year all‑cause death rates in the T1DM and T2DM groups.
Previously diagnosed DM, new‑onset DM, and transient hyperglycemia are associated with adverse outcomes in patients with MI. Hyperglycemia in patients without established DM in the setting of MI may be transient and induced by stress or may be a reflection of an underlying, undiagnosed metabolic syndrome. For many years, the exact definition of stress hyperglycemia has not been established.14,15 In 2019, the American Diabetes Association guidelines described stress hyperglycemia as having a random glucose level greater than 140 mg/dl in critically ill patients without previous DM diagnosis.16 According to this definition, in a recent study, the incidence in STEMI patients was 16.8%.17 Similar to our study, Gencer et al11 defined hyperglycemia as fasting glycemia of at least 10 mmol/l (≥180 mg/dl). Among 3858 patients with ACS, 18.4% had known diabetes, while 3.6% of nondiabetic patients had hyperglycemia on admission.11
Clinical trials indicate a higher‑risk profile for CAD in those with DM compared with those without. A study including 6700 patients with MI showed higher rates of hypertension, history of CAD, MI, and congestive HF in diabetics than in nondiabetics, which is consistent with our findings.18
Our study evaluated differences in therapeutic strategies used to treat patients with transient hyperglycemia or DM compared with the control group. An invasive diagnostic procedure was used in more than 90% of cases in all 5 groups; however, invasive treatment strategies varied per group. As in previously reported studies, invasive diagnostic and therapeutic procedures were less common in patients with either T1DM or T2DM than in non‑DM, transient hyperglycemia, or new‑onset diabetes groups.3 Immediate coronary reperfusion is recommended in all patients with acute STEMI. In high‑risk NSTEMI patients, coronary angiography is recommended within 24 hours of hospital admission.19 Shemesh and Zafir20 showed that diabetes was an independent predictor of late or repeated revascularization and long‑term mortality in very old patients undergoing coronary angiography. Langerqvist et al21 not only emphasized increased post‑PCI survival rates in all patients in general but, more importantly, the improved survival rates in the DM population in particular.
Our findings concur that MVD is more prevalent in patients with T2DM compared with other populations. Some reports state that diabetic patients are more likely to have extensive CAD.18 Our study concluded that T1DM and T2DM groups had higher rates of CABG surgery than the control group due to superiority of CABG over PCI in treatment of MVD both in chronic coronary syndromes22-24 and ACS.25 In a large study, CABG was associated with better outcomes compared with PCI for MVD.25 Importantly, the study showed that patients undergoing CABG (as compared with PCI) had 37% less major adverse cardiac or cerebrovascular events and a 52% reduction in all‑cause death in the long term in patients with and without ACS. In our study, the number of invasive interventions performed in adults with new‑onset diabetes and transient hyperglycemia was similar to that in non‑DM patients.
While analyzing complications in our cohort, we observed the highest bleeding rate in the transient hyperglycemic group, which perhaps was caused by the smaller group size. Our patients with T1DM and T2DM had higher bleeding complication rates compared with nondiabetics. Similarly, the incidence of 30‑day bleeding events in a study by Zhang et al26 was higher for DM patients than nondiabetics (6.2% vs 0.9%; P <0.05). DM is an independent risk factor for post‑MI hemorrhagic complications, and it is one of the 8 parameters assessed via the CRUSADE bleeding risk scale for patients with NSTEMI.27 We observed a tendency for a higher reinfarction rate in DM groups compared with nondiabetics. Giorda et al28 revealed that every year, 6.1% of diabetic patients with a prior cardiovascular event developed a new major atherosclerotic complication. Insulin therapy is a risk stratifier for stent thrombosis and other PCI‑related adverse events.6 Stress hyperglycemia may contribute to the formation of intracoronary thrombus and has been identified as a better predictive value than blood glucose levels on admission.29 Strategies to balance ischemic events and bleeding complications still require further investigation.30
Similarly to previous studies,17,18 our results showed that cardiogenic shock was more common in patients with DM and transient hyperglycemia. The rates of cardiogenic shock in the T2DM group and transient hyperglycemia groups were 1.8% and 1.9%, respectively (vs 1.3% in the control group), but only T2DM was associated with a significantly higher RR of MI complicated by cardiogenic shock. A larger study group would be required for a narrower CI and to obtain statistical significance. According to the TRACE registry, cardiogenic shock develops approximately twice as often in diabetic than in nondiabetic patients with AMI.18 This observation is consistent with a study by Echouffo‑Tcheugui et al3 which covered a major cohort of 1 332 530 hospitalizations for acute MI. A pre‑existing diagnosis of DM increases the risk of cardiogenic shock. Among patients hospitalized for AMI between 2012 and 2014, 5.5% of MI cases were complicated by cardiogenic shock, which occurred more frequently among DM patients.3 Additionally, Khalfallah et al17 reported that MI complicated by cardiogenic shock was more prevalent in the stress hyperglycemia group than in nondiabetics (P = 0.001).
The risk of pulmonary edema in our study was roughly twice as high in all study groups as compared with the control group. This concurs with previous studies. Gencer et al11 showed that among nondiabetic patients hospitalized with ACS, patients with a fasting hyperglycemia of 10 mmol/l or more, compared with nonhyperglycemic patients, were more likely to present with STEMI and acute HF. Patients with DM have a measurably higher risk of acute pulmonary edema compared with those without DM (11% and 4%, respectively).31 The risk of developing HF as a complication after MI was 1.5- to 2‑fold higher in diabetic patients compared with nondiabetics, irrespective of normal left ventricular ejection fraction or previous MI.32 As DM still remains an independent predictor of HF after MI, left ventricular diastolic dysfunction has been suggested to be a potential mechanism resulting in elevated left ventricular filling pressure.33 In a study by Lamblin et al,33 DM was an independent predictor of cardiovascular death or rehospitalization for HF during 1‑year follow‑up. Since stress hyperglycemia presents as an independent predictor for adverse left ventricular remodeling, Shuai et al34 suggested this noninvasive parameter may be used to estimate its risk.
Our study showed no differences between groups in terms of acute mechanical complications. The largest analyses of mechanical complications post‑MI showed that the rates of mechanical complications are low; however, these rates did not improve between 2003 and 2015.35 DM was not a predictor of mortality among patients with mechanical complications.35
Diabetes is associated with an increased in‑hospital3 and long‑term mortality.4-6 In our study, both T1DM and T2DM were independent factors of mortality in long‑term (3‑year) follow‑up, which is consistent with the results of Norhammar et al.36 Long‑term mortality was higher in diabetic patients compared with those without DM and this mortality gap increased with follow‑up time.36 Similarly, in a study by Alabas et al,4 in over 1.94 million person‑years of follow‑up including over 120 000 patients with diabetes, at index AMI, diabetes was associated with significant long‑term excess mortality compared with the effects of comorbidities, risk factors, and cardiovascular treatments. Similarly to Seo et al,37 we found that patients with new‑onset DM did not differ in terms of long‑term prognosis compared with those without DM.
Controversy remains regarding the prognostic value of hyperglycemia in patients without DM hospitalized with MI with regard to long‑term outcomes. Blood glucose measured at admission and fasting glucose have been suggested as useful criteria for triage of nondiabetic ACS, of which the latter is considered beneficial in the long‑term follow‑up.38 Gencer et al11 determined that among nondiabetic patients hospitalized with ACS, a fasting hyperglycemia of at least 10 mmol/l predicted 1‑year mortality. Monteiro et al39 determined that hyperglycemia at admission due to ACS was a short‑term and long‑term negative prognostic marker, particularly in nondiabetic patients, being a strong independent predictor of in‑hospital mortality. The finding that the prognostic impact of admission glycemia and stress hyperglycemia is different in patients with and without previously known diabetes was also confirmed in other studies.11,12,40 Kosiborod et al40 showed that higher admission plasma glucose (APG) levels were associated with elevated 30‑day and 1‑year mortality, in which the nondiabetic group predominated. Similarly, in a study by Ritsinger12 the event rate was the highest in individuals without known diabetes and with APG greater than 11 mmol/l (198 mg/dl), followed by those with established DM. Stress hyperglycemia as an independent predictor of mortality in non‑DM patients was also confirmed in recent studies.17,41
Study strengths and limitations
The strengths of this study include the use of an extensive nationwide prospective cohort of over 58 000 patients with MI hospitalized in Polish hospitals coupled with a uniform set of diagnostic and treatment procedures. Unlike the available English‑language literature, our study is not limited to admission glucose values. Multiple glucose measurements were taken during the acute MI phase and in the following days throughout hospitalization.
Several inherent limitations of the study need to be considered in the interpretation of our findings. Due to the immense size of the data source, the analyzed set of data could potentially include some incomplete or missing information. Moreover, because of the nonrandomized observational design of this study, not all causal relationships or effects of medications on the course of hospitalization or on the prognosis are known. Since data refer to patients hospitalized between 2009 and 2012, there might have been changes in pharmacological and nonpharmacological therapies over the years which could have additional impact on outcomes. The data set of our study cohort, which reflects the proportional distribution of individual conditions in the Polish population, led to considerable differences in the size of individual subgroups, hereby possibly affecting the results of our statistical analyses due to small numbers. The low percentage of the transient hyperglycemia group may be explained as follows. Recent studies defined hyperglycemia as serum glucose in the range between more than 122 mg/dl42 up to more than 198 mg/dl,41 which may have resulted in a diverse distribution of patients per group in these studies. Secondly, a lower proportion of patients without known DM received insulin during hospitalization compared with patients with DM, even with severe hyperglycemia. The insulin administration rates during hospitalization were only 5.6% for patients without diabetes with glycemia between 170 to 240 mg/dl and 21.8% for patients with glycemia of at least 240 mg/dl.40 In addition, new‑onset DM has not been excluded in all studies, which may have resulted in a greater proportion of patients in the transient hyperglycemic group.
Conclusions
Patients with MI and T1DM or T2DM are at a high risk of early‑onset complications and have elevated in‑hospital and long‑term mortality rates. Patients with MI and DM or transient hyperglycemia have a 2‑fold higher risk of pulmonary edema compared with that in nondiabetics. Patients with T2DM or transient hyperglycemia were also more likely to develop cardiogenic shock during hospitalization, but only T2DM was associated with a significantly higher risk of MI complicated by cardiogenic shock. Despite the higher complication and mortality rates in post‑MI diabetic patients, those patients did not differ significantly from their nondiabetic counterparts in terms of the rates of mechanical complications of acute MI. This study highlights important differences (in terms of clinical correlates and outcomes) between patients with transient hyperglycemia and those with different types of DM hospitalized for MI. The findings of this and other relevant studies will increase our understanding of MI occurring in diabetic patients and, ultimately, help develop better treatment strategies and optimize medical care in patients with diabetes.
- Castro MR, Simon G, Cha SS, et al. Statin use, diabetes incidence and overall mortality in normoglycemic and impaired fasting glucose patients. J Gen Intern Med. 2016; 3: 502‑508. | Crossref
- Ofstad AP. Myocardial dysfunction and cardiovascular disease in type 2 diabetes. Scand J Clin Lab Invest. 2016; 76: 271‑281. | Crossref
- Echouffo‑Tcheugui JB, Kolte D, Khera S, et al. Diabetes mellitus and cardiogenic shock complicating acute myocardial infarction. Am J Med. 2018; 131: 778‑786. | Crossref
- Alabas OA, Hall M, Dondo TB, et al. Long‑term excess mortality associated with diabetes following acute myocardial infarction: a population‑based cohort study. J Epidemiol Community Health. 2017; 71: 25‑32. | Crossref
- Norhammar A, Lindbäck J, Rydén L, et al. Improved but still high short- and long‑term mortality rates after myocardial infarction in patients with diabetes mellitus: a time‑trend report from the Swedish Register of Information and Knowledge about Swedish Heart Intensive Care Admission. Heart. 2007; 93: 1577‑1583. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION