Incidental finding of diffuse malignant mesothelioma in the greater omentum during the diagnostic workup of a lung tumor



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Incidental finding of diffuse malignant mesothelioma in the greater omentum during the diagnostic workup of a lung tumor
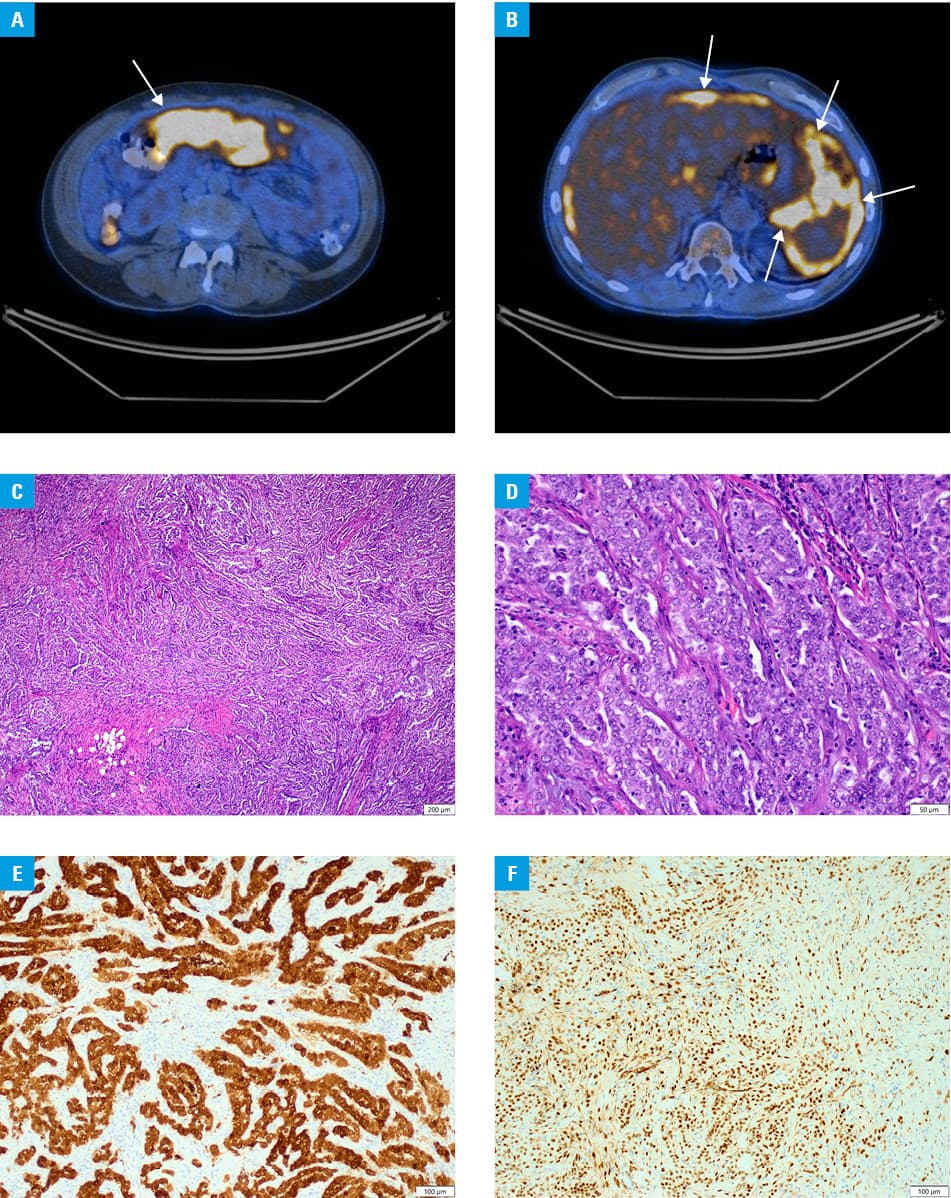
A 60‑year‑old man with no past medical history and a smoking history of 30 pack‑years reported to a surgical clinic with the results of a routine chest radiograph followed by chest computed tomography (CT) presenting a tumor in the left lung (25 × 15 mm). The patient did not notice weight loss nor elevated body temperature in previous months, and further physical examination revealed no abnormalities. Positron emission tomography with CT showed no abnormal 18F‑fluorodeoxyglucose (18F‑FDG) uptake in the tumor. However, multiple nodules in the peritoneum and the greater omentum with elevated 18F‑FDG uptake were visualized. The dominant lesion in the greater omentum was estimated to be the size of 82 × 38 mm (Figure 1A and 1B). Furthermore, metabolically active right subclavicular lymph nodes and the right parasternal lymph node, sized 14 × 11 mm and 8 × 8 mm, respectively, were found. The patient was admitted to the surgery department to undergo an exploratory midline laparotomy with a surgical biopsy from the largest omental lesion. Intraoperatively, a large mass in the greater omentum and multiple small nodular lesions covering the peritoneum, the small intestine, and the greater omentum were exposed. Histopathological examination revealed a tumor composed of epithelioid cells embedded in a desmoplastic stroma. Tumor cells formed tubules, papillary structures, and a few solid groups of cells. A mild to moderate pleomorphism was observed and mitotic activity was low. Immunohistochemical studies demonstrated tumor cells positive for cytokeratins (CK5/6 and CK7) and mesothelial markers (calretinin, WT1, D2‑40) (Figure 1C–1F). The histopathological diagnosis of epithelioid mesothelioma was established. The patient had no known exposure to asbestos in the past. Due to the metastatic stage of the disease, palliative chemotherapy with pemetrexed and cisplatin was introduced. The patient underwent 7 cycles of chemotherapy after which the second positron emission tomography CT was performed. It showed major regression of lesions in the lymph nodes and most of the lesions in the peritoneal cavity. Only some residual lesions (maximum size of 14 mm) in the peritoneum were found. The lung tumor remained stable after treatment and was suggested to be a post‑inflammatory lesion. The patient complained only of a headache persisting since the beginning of treatment. Additional CT detected no abnormalities in the brain. More images are available in Supplementary material.
Malignant peritoneal mesothelioma is a very rare aggressive neoplasm originating from mesothelial cells, with the occurrence estimated between 0.2 and 3 cases per million population per year.1 Mesotheliomas most commonly occur in the pleura, less often in the peritoneum, and are extremely rare in the pericardium or the tunica vaginalis testis.1,2 Malignant peritoneal mesothelioma is reported to represent 20% of all mesotheliomas.2 However, malignant omental mesothelioma is exceptionally unusual, and to our knowledge, there are only a few cases described in the English literature.3 Mesothelioma is commonly associated with asbestos exposure, which is still the most significant risk factor for this disease. However, the percentage of mesotheliomas related to asbestos is decreasing and accounts for approximately 70% to 90% of pleural mesotheliomas, and approximately 50% of peritoneal mesotheliomas. Our knowledge of other risk factors for mesothelioma is expanding with the following distinguished so far: mineral fibers other than asbestos, therapeutic radiation, and recurrent peritonitis and germline mutations. Also, idiopathic mesotheliomas account for a small proportion of cases.4 Histologically, 3 types are distinguished: epithelioid (with the best prognosis), sarcomatoid, and biphasic. Malignant peritoneal mesothelioma in the metastatic stage has a poor prognosis. Therapeutic options include palliative chemotherapy, cytoreductive surgery, and hyperthermic intraperitoneal chemotherapy. Combining cytoreductive surgery and hyperthermic intraperitoneal chemotherapy is said to prolong survival.5
The diagnosis of a malignant mesothelioma in the greater omentum is unexpected, since metastases are the most common tumors of the greater omentum, while primary tumors in this location are very rare. However, when a diffuse lesion in the peritoneal cavity is encountered, a mesothelioma should be considered.
- Salo SAS, Ilonen I, Laaksonen S, et al. Epidemiology of malignant peritoneal mesothelioma: a population‑based study. Cancer Epidemiol. 2017; 51: 81‑86. | Crossref
- Hassan R, Alexander R, Antman K, et al. Current treatment options and biology of peritoneal mesothelioma: meeting summary of the first NIH peritoneal mesothelioma conference. Ann Oncol. 2006; 17: 1615‑1619. | Crossref
- Minami K, Okumura H, Hiwatashi K, et al. Multiple malignant epithelioid mesotheliomas of the liver and greater omentum: a case report and review of the literature. Surg Case Rep. 2017; 3: 66. | Crossref
- Attanoos RL, Churg A, Galateau‑Salle F, et al. Malignant mesothelioma and its non‑asbestos causes. Arch Pathol Lab Med. 2018; 142: 753‑760. | Crossref
- Salo SAS, Ilonen I, Laaksonen S, et al. Malignant peritoneal mesothelioma: treatment options and survival. Anticancer Res. 2019; 39: 839‑845. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION