A 25‑year‑old Caucasian woman, who was in generally good health, developed a lump in the left popliteal fossa (Figure 1A). The patient was admitted to a hospital due to excruciating pain in the lower leg with additional paresthesia on the posterolateral side of the left ankle. Other systemic diseases or taking any medications were excluded.
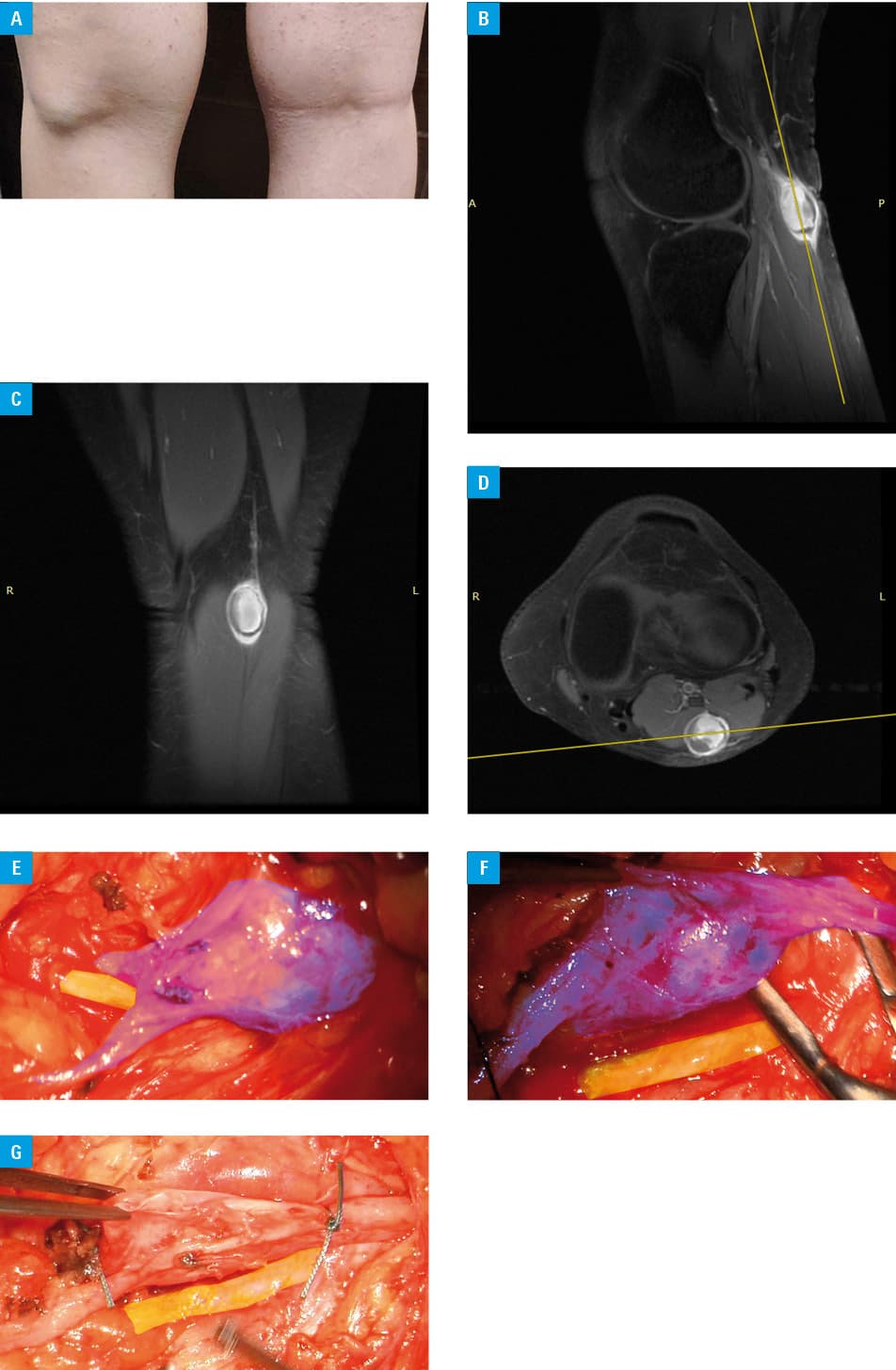
Magnetic resonance imaging (MRI) revealed a heterogeneous focal lesion (1.6 cm × 1.5 cm × 2.2 cm) located peripherally in the left popliteal fossa, in the subcutaneous tissue between the medial and lateral head of the gastrocnemius muscle. The lesion slightly compressed adjacent muscles (Figure 1B–1D). Its internal part was mostly filled with blood in the methemoglobin phase. The lesion sack was quite wide and enhanced after contrast administration. The MRI images were assessed as indicative of a tibial nerve neuroma complicated by bleeding. Ultrasonographic examination of the left lower limb vessels revealed that the proximal part of the left short saphenous vein was distended and widened (1.7 cm × 1.1 cm × 2.5 cm; Supplementary material, Figure S1A–S1D). The lesion with a heterogeneous focus of 1.2 cm × 0.8 cm × 0.7 cm was visible in the vein lumen and was connected to the anterolateral part of the vessel wall. The lesion was most clearly visible in a vertical position. Such an unusual clinical manifestation could correspond to a thrombus or perhaps a benign tumor in the wall of the short saphenous vein.
An S‑shaped skin incision was made in the left popliteal fossa. After dissecting the tissues, the lateral sural cutaneous nerve was exposed. Next, the short saphenous vein varicose compressing the nerve was visualized (Figure 1E). These structures were surgically separated using blunt dissection (Figure 1F). An incision was made in the short saphenous vein wall with the evacuation of the thrombus. Finally, the vein abnormal segment was ligated (Figure 1G). This lesion could mimic the tibial nerve neuroma on MRI (Figure 1B–1D), all the more so because this anomaly was closely related to the nerve posterior aspect.
Varicose veins are quite a common condition, frequently associated with particular risk factors such as female sex, pregnancy, obesity, menopause, aging, prolonged standing, or leg injury. This condition can lead to many symptoms, for example, pain, ankle swelling, and restless leg syndrome. Interestingly, anomalous veins or venous malformations located along the course of the sciatic nerve or its branches may lead to significant symptoms along the territory of the nerves. These symptoms may include pain, itching, heaviness, and tingling.1
To the best of our knowledge, the presented report is the first published clinical case of a varicose vein mimicking neuroma. All currently available PubMed records pertaining to varicose veins and neuromas focus on rare complications in the surgical treatment of varicose veins.2-4 We believe that this publication may be helpful in the diagnostic process and treatment planning of similar cases.
- Labropoulos N, Tassiopoulos AK, Gasparis AP, et al. Veins along the course of the sciatic nerve. J Vasc Surg. 2009; 49: 690‑696. | Crossref
- Simonetti S, Bianchi S, Martinoli C. Neurophysiological and ultrasound findings in sural nerve lesions following stripping of the small saphenous vein. Muscle Nerve. 1999; 22: 1724‑1726. | Crossref
- Giannas J, Bayat A, Watson SJ. Common peroneal nerve injury during varicose vein operation. Eur J Vasc Endovasc Surg. 2006; 31: 443‑445. | Crossref
- Ahuja A, Grant T, Dumanian G, Resnick SA. Development of traumatic neuromas in a patient following endovenous laser ablation and microphlebectomy procedures: a rare complication from the removal of varicose veins. Cureus. 2021; 13: 1‑5. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION