The role of antithyroid antibodies in thyroid dysfunction after allogeneic hematopoietic stem cell transplantation

 CC BY 4.0
CC BY 4.0
The role of antithyroid antibodies in thyroid dysfunction after allogeneic hematopoietic stem cell transplantation
Introduction
Despite availability of the newest, highly effective drugs in hematology, the number of allogeneic hematopoietic stem cell transplantations (alloHSCTs) performed in Europe is constantly growing, having reached 45 364 in 2020.1
Unfortunately, alloHSCT is associated with many adverse consequences. Traditionally, they are divided into early (≤100 days) and late (>100 days after alloHSCT) events. There is a plethora of late complications that may lead to a considerable decrease in the quality of life and, in some cases, to death. Among them are ocular, pulmonary, cardiovascular, dermatologic, neurologic, skeletal, gastrointestinal, and urologic dysfunctions, secondary neoplasms, as well as endocrine complications.2
Impairment of the endocrine function following alloHSCT can be associated with previous therapies, graft‑vs‑host disease, and exposure to corticosteroids after the procedure.3 Particularly well known is thyroid dysfunction, with subclinical hypothyroidism being the most frequently diagnosed.4 In the literature, the incidence of subclinical hypothyroidism 12 to 18 months after alloHSCT reaches 12% to 15%.5 Therefore, the consensus recommendations advise checking the thyroid function yearly after alloHSCT, or every time a dysfunction is suspected.6
Of note, in patients referred for alloHSCT, thyroid dysfunction may exist before the procedure. Frequently, even though the level of thyroxine (T4) is decreased (sometimes along with the level of free thyroxine [FT4]), and the level of thyroid‑stimulating hormone (TSH) is increased, the patients do not show symptoms of hypothyroidism. Such impairment of the thyroid function is typical of chronic diseases.
The aim of this study was to evaluate the prevalence of subclinical and clinical thyroid dysfunctions before as well as 3 months and 1 year after alloHSCT. Moreover, the presence of antithyroid antibodies before and after alloHSCT was evaluated.
Patients and methods
We performed a prospective, observational, noninterventional analysis of patients after alloHSCT transplanted between March 2012 and January 2016 at the Department of Hematology, Transplantation, and Internal Medicine; University Clinical Center of the Medical University of Warsaw, Poland. The thyroid function tests were conducted before (within 1 week before the beginning of conditioning) as well as 3 months (83–100 days) and 1 year (367–380 days) after alloHSCT. The day of alloHSCT was marked as day 0 in the study. All the procedures were standard and performed routinely in all patients before and after alloHSCT. The Bioethics Committee was informed about the beginning of the study, and approval was not required. The patients were included before they underwent alloHSCT. Information regarding patient characteristics was collected retrospectively from medical records (data before alloHSCT) and prospectively (data from the moment of patient inclusion in the study). The study was conducted in accordance with the Helsinki Declaration.
The thyroid function test results for TSH, free triiodothyronine (FT3), FT4, antithyroid peroxidase (anti‑TPO), and thyroglobulin antibodies (anti‑TG) before alloHSCT were available in 173 patients. Hypothyroidism was diagnosed in the patients with high levels of TSH (>4.2 mIU/l) and decreased levels of FT3 (<3.1 pmol/l) and / or FT4 (<12 pmol/l). Subclinical hypothyroidism was diagnosed in the patients with TSH levels above 4.2 mIU/l and with normal FT3 (3.1–6.8 pmol/l) and FT4 (12–22 pmol/l) concentrations. Hyperthyroidism was diagnosed in the patients with TSH levels below 0.27 mIU/l and increased levels of free hormones (FT4 >22 pmol/l and / or FT3 >6.8 pmol/l). Subclinical hyperthyroidism was considered present in the patients with TSH levels below 0.27 mIU/l and with normal concentrations of free hormones (FT3, 3.1–6.8 pmol/l and FT4, 12–22 pmol/l).
Patients were included in the group with antithyroid antibodies when anti‑TPO concentrations were above 34 IU/ml or anti‑TG levels were above 115 IU/ml.
Statistical analysis
The statistical analysis was conducted using the R software v.4.1.1 (IDE RStudio v.1.4.1717, R Foundation for Statistical Computing, Vienna, Austria). The study groups were characterized using descriptive statistics (medians, ranges). The influence of antithyroid antibodies measured before alloHSCT on the frequency of subclinical hypothyroidism after the procedure was assessed with the Fisher exact test. To check whether the distribution was uniform, the χ2 test was used. The associations between thyroid function test variables and parameters related to patient characteristics and transplantation were calculated using the Pearson correlation coefficient. The tests were considered significant if P was below 0.05.
Results
Results of thyroid function tests before, 3 months after, and 1 year after allogeneic hematopoietic stem cell transplantation
Among the 173 consecutive patients whose thyroid function was assessed before alloHSCT, abnormalities were found in 59 individuals (33.53%), and the majority of them (n = 54 [31.21%]) had subclinical hypothyroidism. However, none of the patients was diagnosed with hypothyroidism with clinical manifestation within the week before the start of conditioning. Six patients (3.4%) received levothyroxine because of hypothyroidism diagnosed long before alloHSCT. Five of them (2.9%) reached euthyreosis before the transplantation. One patient had an increased TSH concentration along with normal levels of free thyroid hormones. Hyperthyroidism was diagnosed in 1 patient (0.58%), and subclinical hyperthyroidism in 3 (1.73%).
Three months after alloHSCT, thyroid function tests were performed in 157 patients, and abnormalities were found in 51 of them (32.48%). In 43 patients (27.39%), features of subclinical hypothyroidism were noted, and 1 patient (0.64%) was diagnosed with overt hypothyroidism. Three patients received levothyroxine and were in euthyreosis. None of the patient were diagnosed with hyperthyroidism. Subclinical hyperthyroidism was diagnosed in 2 patients (1.27%), and features of low FT3 syndrome were noted in 5 individuals (3.18%).
One year after alloHSCT, the thyroid function was evaluated in 87 patients, and abnormalities were found in 11 of them (12.64%). Nine patients (10.34%) were diagnosed with subclinical hypothyroidism, and in 2 individuals (2.3%) features of subclinical hyperthyroidism were observed. Of note, none of the patients was diagnosed with hypo- or hyperthyroidism. Two individuals received levothyroxine and were in euthyrosis.
Overall, 76 patients had the thyroid function assessed at all 3 time points. In this group, only 3 persons (4%) were diagnosed with subclinical hypothyroidism before and after alloHSCT. In 1 patient, antithyroid antibodies were detectable at every time point, whereas the 2 other patients were not tested for the presence antithyroid antibodies. Interestingly, 14 patients (18.4%) with subclinical hypothyroidism diagnosed before alloHSCT were in euthyrosis 1 year after the transplantation. Additionally, only half of them (n = 7) had subclinical hypothyroidism 3 months after alloHSCT. None of them received levothyroxine. In 5 patients who were in euthyrosis before alloHSCT, subclinical hypothyroidism occurred 3 months after the transplantation, but after 1 year the thyroid function returned to normal. One patient was diagnosed with hyperthyroidism before alloHSCT, and he was negative for antithyroid antibodies before and after the procedure. After starting therapy with thiamazole, that patient remained in euthyrosis during the follow‑up.
Fourty‑six patients (60.5%) remained in euthyrosis during the entire follow‑up. Interestingly, 21 of them were tested for the presence of antithyroid antibodies before alloHSCT, and the results were positive in 3 individuals (6.5%) (Supplementary material, Table S1).
Analysis of antithyroid antibodies before and after allogeneic hematopoietic stem cell transplantation
Before alloHSCT, the levels of antithyroid antibodies were tested in 142 patients. The results were strongly positive in 19 patients (13.4%), including 7 individuals (4.9%) with high concentrations of anti‑TG antibodies, 10 (7%) with high levels of anti‑TPO antibodies, and 2 (1.4%) with high concentrations of both antibody types. The median levels of anti‑TG and anti‑TPO antibodies before alloHSCT were 22.13 IU/ml (range, 1–4200 IU/ml) and 31.85 IU/ml (range, 3–650 IU/ml), respectively.
Three months after alloHSCT, the levels of antithyroid antibodies were tested in 35 patients. In this group, high concentrations of antibodies were detected in 8 patients (22.86%). Among them, 4 patients (11.4%) had a high anti‑TG concentration, 1 (2.85%) had a high level of anti‑TPO antibodies, and 3 patients (8.6%) had high concentration of both antibody types. The median concentration of anti‑TG antibodies was 100.9 IU/ml (range, 5–4500 IU/ml), and the median level of anti‑TPO was 15.32 IU/ml (range, 3–563.7 IU/ml).
One year after alloHSCT, the antithyroid antibody levels were tested only in 13 patients. In this group, the antibody titer was high in 4 individuals (30.77%), including 2 (16.7%) with a high concentration of anti‑TG and 2 with increased levels of both antibody types. The median anti‑TG antibody level was 518.7 IU/ml (range, 5–4500 IU/ml), whereas for anti‑TPO antibodies, it was 11.59 IU/ml (range, 3–350.5 IU/ml) (Figure 1).
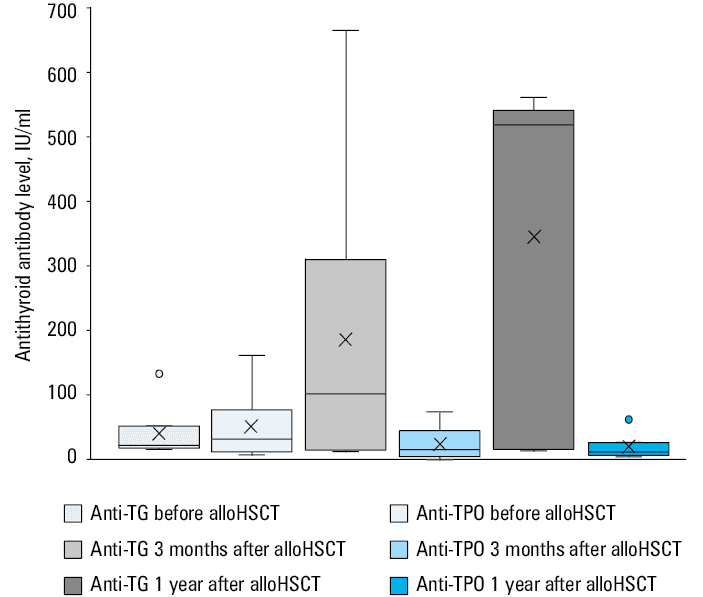
Abbreviations: anti‑TG, thyroglobulin antibodies; anti‑TPO, thyroperoxidase antibodies
A total of 34 patients had the antithyroid antibody titers measured before and after alloHSCT. In the group of patients with a high titer of antithyroid antibodies before transplantation (n = 11 [32.4%]), the percentage of patients with subclinical hypothyroidism after alloHSCT was significantly higher than in the group with a low titer of antithyroid antibodies before alloHSCT (n = 9 [82%] vs n = 6 [26.1%]; P = 0.004). In the patients with high antibody titers determined 3 months after alloHSCT (n = 8), subclinical hypothyroidism was significantly more common than euthyroidism (n = 6 [75%] vs n = 2 [25%]; P = 0.042).
Discussion
Based on the previous studies, the incidence of thyroid dysfunction after HSCT ranges between 20% and 58%.3,6-8 In our study, before the procedure, thyroid function disorders occurred in 59 patients (33.3%), including 54 patients (31.21%) with features of subclinical hypothyroidism. According to the literature, subclinical hypothyroidism is the most common pathology of this gland. Some authors state that subclinical hypothyroidism usually occurs in the early period after transplantation, with the peak incidence around 100 days after alloHSCT.5,9 Twelve to 18 months after transplantation, the incidence ranges between 12% and 15%. However, it may also develop later.5,9 In a study by Somali et al,10 subclinical hypothyroidism was detected in approximately 13% of patients within 18 months of alloHSCT. In a single‑center study involving 791 patients, new cases of thyroid disease were noted even more than 20 years after transplantation.11
In the present study, in a selected group of participants with thyroid function tests performed at all time points (n = 76), subclinical hypothyroidism was diagnosed in 22.4% of the patients before transplantation, 25% of the patients 3 months after alloHSCT, and 10.5% of the patients 1 year after the procedure. These results do not differ substantially from those obtained in other reports. The decrease in the percentage of patients with subclinical hypothyroidism in the period after transplantation, also observed in other studies, is noteworthy.5,9 None of the patients included in this group had been treated with levothyroxine. This suggests that the increase in TSH levels 3 months after alloHSCT in some persons may be associated with the response of the pituitary gland to recovery from the disease. This is indicated by an increase in the levels of other gonadotropins (luteinizing hormone and follicle‑stimulating hormone) simultaneously with the increase in TSH in 62% of the patients with test results available 3 months after the transplantation (data not shown). In addition, attention should be paid to the potential impact of medications on the test results. In patients receiving glucocorticoids, for instance due to graft‑vs‑host disease, peripheral conversion of T4 to T3 as well as TSH and FT3 levels may decrease, with normal FT4 levels (most of the plasma T3 pool comes from peripheral conversion, that is, 5′-deiodination of thyroxine) as a result of the inhibitory effect of glucocorticosteroids on thyrotropin secretion.12
The implementation of levothyroxine therapy in patients with subclinical hypothyroidism is controversial. While most authors agree that TSH levels above 10 mIU/l are associated with symptoms of overt hypothyroidism, regardless of the FT4 and FT3 levels, and recommend starting treatment in such cases, the opinions are divided on whether to treat patients with subclinical hypothyroidism with a TSH level of 5 to 10 mIU/l.6 In the general population with subclinical hypothyroidism, when deciding on the implementation of levothyroxine treatment, an individual approach to the patient is recommended, taking into account factors such as the presence of goiter, therapeutic attempts to eliminate the possible symptoms of hypothyroidism, patient preference, presence of antithyroid antibodies, TSH concentration above 8 mIU/l on 2 measurements, progressive increase in TSH level, bipolar affective disorder, depression, infertility, ovulatory disorders, young age, hyperlipidemia, childhood, and pregnancy or intention to become pregnant.13 Literature data on the general population indicate that there is a risk of subclinical hypothyroidism complications, which is reduced after treatment with levothyroxine. For instance, there is an increase in the risk of cardiovascular mortality14; in patients with subclinical hypothyroidism it may be 41% higher than in the euthyroid control group,15 especially among people younger than 65 years.16 Given the fact that individuals referred for alloHSCT are frequently younger than 70 years and that the cardiovascular risk after the procedure is considerably increased, it should be recommended to treat the patients with TSH levels above 5 mIU/l. That recommendation is particularly justified in the group with antithyroid antibodies present before the transplantation—this factor may help identify patients with higher risk of maintaining subclinical hypothyroidism after alloHSCT.
Other possible complications of untreated subclinical hypothyroidism include exacerbation of depression or bipolar disorder, disorders of the muscle function, neuronal conduction, cardiac function, as well as cognitive and mental functions.17 Moreover, one of the arguments for the implementation of levothyroxine treatment in the patients after alloHSCT is an increased risk for developing papillary thyroid cancer.18
Patients with subclinical hypothyroidism and positive antithyroid antibody titers are at risk of clinically overt hypothyroidism.19 In the study by Somali et al10 conducted in a group of 72 patients after alloHSCT without previous thyroid diseases, hypothyroidism was diagnosed in 6% of men and 5% of women within 18 months of the transplantation.10 In the present study, no patient was diagnosed with clinically overt hypothyroidism in the pretransplantation period. Five patients had been diagnosed with that entity earlier—they had been receiving substitution treatment and the TSH concentration in the peritransplantation period was normal. After alloHSCT, clinically overt hypothyroidism was detected in 1 patient. The small percentage of patients with hypothyroidism is most likely related to the short (1‑year) follow‑up.
Based on the current observations, in some individuals, the thyroid function normalizes without treatment. In the present study, normalization of the TSH level 1 year after the transplantation in patients with subclinical hypothyroidism diagnosed before and / or 3 months after alloHSCT was observed in 20 patients, which constitutes 26.3% of all participants, and 86% of those with subclinical hypothyroidism diagnosed during the peritransplant period and 3 months after alloHSCT. It is noteworthy that among the participants whose TSH levels normalized after a year, only 1 patient had a positive antithyroid antibody titer. On the other hand, in the patients diagnosed with subclinical hypothyroidism after 1 year, a high titer of antithyroid antibodies in the peritransplantation period was detected in almost all persons in whom this test was performed. This significantly supports the role of checking the levels of antithyroid antibodies before alloHSCT and starting treatment with levothyroxine in the individuals with positive antibody titers.
Conclusions
Antibodies seem to be a valuable marker that can help distinguish patients with subclinical hypothyroidism from those with high TSH levels due to a chronic disease. This differentiation seems to play an important role. In the majority of patients with increased TSH levels before alloHSCT, the concentration of this hormone returned to normal 1 year after the procedure. However, some patients (especially those with positive antibody titers before alloHSCT) maintained subclinical hypothyroidism for 1 year after the transplantation, which may contribute to an increased risk of cardiovascular diseases and other complications. These observations highlight the importance of checking the levels of antithyroid antibodies during patient qualification for alloHSCT, because the results could drive the treatment of subclinical hypothyroidism.
- Passweg JR, Baldomero H, Chabannon C, et al. Impact of the SARS‑CoV‑2 pandemic on hematopoietic cell transplantation and cellular therapies in Europe 2020: a report from the EBMT activity survey. Bone Marrow Transplant. 2022; 57: 742‑752. | Crossref
- Carreras E, Dufour C, Mohty M, Kroger N, eds. The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies. 7th ed. Cham (CH); 2019. | Crossref
- Saunders IM, Tan M, Koura D, Young R. Long‑term follow‑up of hematopoietic stem cell transplant survivors: a focus on screening, monitoring, and therapeutics. Pharmacotherapy. 2020; 40: 808‑841. | Crossref
- Ataca Atilla P, Akkus E, Atilla E, et al. Thyroid dysfunctions in adult patients after allogeneic hematopoietic stem cell transplantation. Clin Transplant. 2020; 34: e14049. | Crossref
- Sklar C, Whitton J, Mertens A, et al. Abnormalities of the thyroid in survivors of Hodgkin’s disease: data from the Childhood Cancer Survivor Study. J Clin Endocrinol Metab. 2000; 85: 3227‑3232. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION