Systematic review and meta-analysis of the safety and efficacy of transvenous lead extraction in octogenarian patients
Key words: cardiac implantable electronic devices, elderly, lead extraction, octogenarian, procedural outcomes

 CC BY 4.0
CC BY 4.0
Systematic review and meta-analysis of the safety and efficacy of transvenous lead extraction in octogenarian patients
Introduction: As the global population ages and the use of cardiac implantable electronic devices increases, transvenous lead extraction (TLE) is being performed more frequently in elderly patients. Concerns remain regarding its safety and efficacy in octogenarians, and age‑specific recommendations are limited.
Objectives: We aimed to assess procedural success, complication rates, and mortality associated with TLE in patients aged 80 years or older in comparison with younger individuals.
Patients and methods: A systematic search of PubMed, Cochrane CENTRAL, SciELO, and ScienceDirect was conducted up to December 2024. Studies reporting TLE outcomes in octogenarians and younger patients were included according to predefined criteria. A meta‑analysis was performed to compare procedural success, complications, and mortality between the age groups.
Results: Seventeen studies including 15 984 patients were analyzed. Complete lead extraction success was 96.7% in octogenarians and 96.2% in the patients aged below 80 years. No significant differences were observed in major or minor procedural complications. In‑hospital mortality was low and comparable between the groups. Although long‑term mortality was higher in the octogenarians, this reflected greater baseline comorbidity and frailty rather than increased procedural risk. None of the included studies demonstrated higher periprocedural danger of TLE in elderly patients.
Conclusions: TLE is safe and effective in patients aged 80 years and older, with outcomes comparable to younger individuals. Advanced age alone should not preclude referral for lead extraction.
What's new?
This systematic review and meta‑analysis offers an updated and robust evaluation of transvenous lead extraction in patients aged 80 years and older. The findings demonstrate that high procedural success can be achieved in this age group without an excess risk of periprocedural complications or in‑hospital mortality when compared with younger individuals. These results counter the assumption that advanced age alone predisposes patients to poor procedural outcomes and emphasize the importance of individualized clinical assessment rather than chronological age. Although long‑term mortality remains higher among octogenarians, this appears to reflect underlying frailty and comorbid conditions rather than procedural factors. Future studies should prioritize frailty‑based risk stratification and optimized care pathways for elderly patients.
Introduction
One of the most significant demographic trends of the 21st century is the progressive aging of the population, largely driven by improvements in medical care and reductions in mortality.1-3 Cardiac arrhythmias remain a major cause of morbidity and mortality in industrialized countries.4,5 The increasing prevalence of bradyarrhythmias and tachyarrhythmias has led to a growing use of cardiovascular implantable electronic devices (CIEDs). As the population ages and more elderly patients undergo device implantation, the number of patients requiring transvenous lead extraction (TLE) continues to rise.6,7
Lead extraction is defined as the removal of any transvenous lead implanted for more than 1 year, a lead requiring specialized extraction tools beyond standard implant equipment, or a lead removed via a route different from the original implant vein.8 Various techniques are available for TLE, including simple traction and the use of dedicated extraction tools, such as locking stylets and powered or mechanical sheaths.9 In contemporary practice, extraction strategies are tailored to the clinical scenario, and different tools are often used interchangeably when necessary to achieve procedural success.10
The most common indication for TLE is device‑related infection, which carries a substantial risk of morbidity and mortality, and constitutes a mandatory indication for complete system removal.11,12 Recent registry data further emphasize the prognostic importance of definite and possible CIED‑related infective endocarditis in this population.13 Additional indications include lead malfunction, venous occlusion, thromboembolic complications, or system upgrades.14-16
Large registries, including the European Lead Extraction Controlled Registry, have demonstrated high overall procedural success rates of over 95% and acceptable complication rate of 1.7% in the general population.17,18 Elderly patients are traditionally considered at a higher procedural risk due to frailty, comorbidities, and reduced physiological reserve.16,19 Consequently, clinicians may hesitate to refer older individuals for TLE, fearing increased rates of major complications or reduced procedural success. However, available evidence addressing the safety and efficacy of TLE specifically in elderly populations remains fragmented, and no clear consensus exists regarding risk stratification and management in this age group.20,21
The overarching goal of this review was to support the clinical decision‑making process by identifying whether advanced age alone should be considered a limiting factor for performing TLE.
Objectives
The primary objective of this systematic review and meta‑analysis was to comprehensively evaluate the safety and efficacy of TLE in octogenarian patients (aged ≥80 y) in comparison with younger individuals (<80 y), using data published up to December 2024.
Specifically, the following research questions were addressed: 1) What are the rates of complete procedural success in patients aged 80 years or older undergoing TLE vs those below 80 years? 2) What is the incidence of major and minor complications associated with TLE in the elderly and younger populations? 3) What is the short‑term (≤30 days) and long‑term mortality following TLE in octogenarians and younger patients? 4) Which TLE techniques are most commonly used (eg, manual traction, mechanical sheath, laser sheath) in octogenarians, and do their frequencies differ significantly from younger patients? 5) Are there any differences in lead characteristics and procedural parameters, such as atrial, right ventricular, and coronary sinus lead removal or lead dwell time across the age groups? and 6) Do infectious vs noninfectious indications or patient comorbidities affect TLE outcomes in octogenarians?
Patients and methods
Protocol and registration
This systematic review and meta‑analysis was prospectively registered in the International Prospective Register of Systematic Reviews database under registration number CRD420250635750. The full registration record is publicly accessible at: https://www.crd.york.ac.uk/PROSPERO/view/CRD420250635750. The protocol outlines the aim to assess the safety and efficacy of TLE in octogenarian patients (aged ≥80 y).
Eligibility criteria
Studies were selected based on predefined inclusion and exclusion criteria formulated according to the PICOS (Population, Intervention, Comparison, Outcomes, Study design) framework. The following inclusion criteria were employed: 1) population: adult patients aged 80 years or older undergoing TLE, either exclusively or in comparison with younger populations; 2) intervention: TLE procedures, regardless of indication (infectious or noninfectious), device type (CIED, pacemaker, implantable cardioverter‑defibrillator [ICD], cardiac resynchronization therapy [CRT]), or extraction technique; 3) comparison: patients aged below 80 years undergoing TLE, or age‑stratified outcome reporting (eg, <80 vs ≥80 y); 4) outcomes: studies reporting at least 1 safety or efficacy outcome, including but not limited to: procedural success (complete or clinical); procedural mortality; complication rate (major / minor); in‑hospital or follow‑up mortality; 5) study design: randomized controlled trials, prospective and retrospective cohort studies, or large case series with at least 10 patients aged 80 years or older; 6) publication type: peer‑reviewed full‑text articles published in English.
The exclusion criteria comprised: 1) case reports, narrative and systematic reviews, editorials, other meta‑analyses, expert opinions, letters to the editor; 2) conference abstracts without sufficient data for analysis; 3) studies in which the mean / median age was below 80 years and subgroup data for octogenarians were not separately available; 4) studies not reporting any TLE‑related outcomes (safety or efficacy); 5) duplicate publications (only the most complete dataset included).
Information sources
A comprehensive systematic literature search was performed across the following electronic databases: PubMed (U.S. National Library of Medicine), CENTRAL (Cochrane Central Register of Controlled Trials), SciELO (Scientific Electronic Library Online), and ScienceDirect (Elsevier Science). The last search was conducted in December 2024. The reference lists of included articles were also hand‑searched to identify any additional relevant studies.
Search strategy
The search strategy was tailored to each database, using appropriate Boolean logic and Medical Subject Headings where applicable. The primary search terms included combinations of: 1) condition and intervention: “lead,” “lead extraction,” “transvenous lead extraction;” 2) population: “octogenarian,” “elderly;” 3) device‑related terms: “CIED,” “pacemaker,” “ICD,” “CRT.”
The applied syntax was: (lead OR lead extraction OR transvenous lead extraction) AND (octogenarian OR elderly) AND (CIED OR pacemaker OR ICD OR CRT).
A detailed breakdown of search results by database up to December 2024 is shown in Table 1.
Database | Search terms used | Records found |
Abbreviations: CIED, cardiac implantable electronic device; CRT, cardiac resynchronization therapy; ICD, implantable cardioverter‑defibrillator | ||
PubMed | (lead OR lead extraction OR transvenous lead extraction) AND (octogenarian OR elderly) AND (CIED OR pacemaker OR ICD OR CRT) | 6440 |
SciELO | (lead OR lead extraction OR transvenous lead extraction) AND (octogenarian OR elderly) AND (CIED OR pacemaker OR ICD OR CRT) | 0 |
CENTRAL | (lead OR lead extraction OR transvenous lead extraction) AND (octogenarian OR elderly) AND (CIED OR pacemaker OR ICD OR CRT) | 65 |
ScienceDirect | (lead OR lead extraction OR transvenous lead extraction) AND (octogenarian OR elderly) AND (CIED OR pacemaker OR ICD OR CRT) | 24 442 |
All identified records were imported into a Mendeley Reference Manager Version 2.130.2 management system and screened for eligibility. The detailed flow of study selection is presented in Supplementary material, Figure S1.
Selection process
Two independent reviewers (GD and KP) performed the study selection in a 2‑step process. First, titles and abstracts were screened for eligibility based on predefined inclusion and exclusion criteria. In the second step, full texts of relevant articles were assessed for eligibility. If necessary, a third reviewer (DJ) was consulted to arbitrate unresolved disagreements. The entire selection process was conducted using Microsoft Excel without automation tools. A PRISMA‑compliant flow diagram was constructed to document the number of studies included and excluded at each stage of the review process.
Data extraction process
Data from the included studies were extracted independently by 2 reviewers using a standardized Excel‑based data collection form developed for the purpose of this study. If relevant data were missing or unclear, the study authors were not contacted for clarification and the variable was excluded from the pooled analysis.
Outcomes
Primary outcomes
The primary outcomes of this systematic review and meta‑analysis were focused on the safety and efficacy of TLE in octogenarian patients (≥80 y), compared with those aged below 80 years. The following aspects were analyzed in detail: 1) complete procedural success, defined according to the 2017 Heart Rhythm Society expert consensus11 as the removal of all targeted leads and lead material from the vascular space without any permanently disabling complications or procedure‑related death; 2) major complications, including events such as cardiac tamponade, vascular laceration, the need for surgical intervention, stroke, or death directly attributed to the extraction procedure; 3) minor complications, such as minor bleeding, hematoma, pneumothorax not requiring intervention, or lead migration not requiring reintervention; 4) short‑term mortality, defined as all‑cause death occurring during hospitalization or within 30 days following the TLE procedure; 5) long‑term mortality, defined as all‑cause death reported during postdischarge follow‑up (when available).
Secondary outcomes
To explore additional dimensions of TLE safety, performance, and context of use in elderly patients, the following secondary outcomes were included: the use of different extraction techniques, lead‑related characteristics, indications for TLE stratified into infectious and noninfectious causes, and patient baseline characteristics stratified by age group. The outcomes were extracted separately for patients aged below and over 80 years. In the studies reporting event counts and group totals, odds ratios (ORs) and 95% CIs were calculated and pooled using random‑effects models. Continuous variables were reported as mean differences (MDs) where applicable.
Risk of bias assessment
The methodological quality and potential risk of bias of the included nonrandomized studies were analyzed using the Newcastle–Ottawa Scale (NOS). This validated tool evaluates 3 broad domains: selection of the study groups (0–4 stars), comparability of the groups (0–2 stars), and ascertainment of either the exposure or outcome of interest (0–3 stars). Each study could therefore receive a maximum score of 9 stars.
The NOS was applied independently by 2 reviewers (GD and KP) who were trained in bias evaluation methodology. Any disagreements were resolved through consensus, with consultation from the third author (DJ) when necessary. The results of the NOS assessments for each study are provided in Supplementary material, Table S1. Studies scoring 7–9 stars were considered at a low risk of bias, 4–6 stars at a moderate risk, and 0‑3 stars at a high risk.
Data synthesis
All meta‑analyses were conducted using a random‑effects model justified by the clinical and methodological heterogeneity across studies. The DerSimonian and Laird method was applied to estimate between‑study variance (τ2). The OR was used as the summary statistic for binary outcomes, while MD was applied for continuous data (eg, time from implantation to extraction). Statistical heterogeneity was assessed using: I2 statistic, representing the percentage of total variation across studies due to heterogeneity rather than chance; τ2, the between‑study variance; and Cochran Q test, with P values indicating significance of heterogeneity. All calculations and plots were performed in R (R Foundation for Statistical Computing, Vienna, Austria) using the “meta” package. Potential publication bias was evaluated using visual inspection of funnel plots and the Egger regression test, with results reported in Supplementary material, Table S2. This represents a limitation of the study. While most outcomes included a sufficient number of studies (eg, >10) to allow for bias assessment, formal tests should be included in subsequent updates or supplementary analyses.
For each variable, the number of events and the corresponding total population were extracted for both age groups. ORs with 95% CIs were calculated to assess the likelihood of the condition being present in older (≥80 y) vs younger (<80 y) patients.
Forest plots were generated to visually summarize comparisons between the octogenarians and younger patients across selected procedural characteristics, clinical outcomes, and technical aspects of TLE. A random‑effects model was applied to calculate pooled effect estimates. Statistical heterogeneity was assessed using standard heterogeneity statistics.
In the forest plots, individual study estimates are represented by squares proportional to study weight, while the diamond represents the pooled effect estimate with its 95% CI.
Results
Population characteristics
The included studies were published between 2011 and 2023 and originated from 9 countries. In total, 15 984 patients underwent TLE, of whom 2823 were aged 80 years or older. Table 2 summarizes the key characteristics of the included studies evaluating TLE in patients aged below and above 80 years. The complete lead extraction success rate is reported separately for both age groups. Furthermore, the number of patients with pacemakers and ICDs is stratified by age. In studies that reported lead types rather than device numbers, descriptive information is included accordingly. Table 3 presents the distribution of key clinical characteristics and comorbidities in patients undergoing TLE stratified by age group (<80 vs ≥80 y). The total number of patients in each age category was 11 396 and 14 880, respectively. Patients aged 80 years or older were found to have a significantly higher prevalence of several comorbidities, including chronic kidney disease (CKD; OR, 3.8; 95% CI, 3.52–4.1), coronary artery disease (CAD; OR, 4.2; 95% CI, 3.92–4.49), chronic obstructive pulmonary disease (COPD; OR, 7.69; 95% CI, 6.35–9.31), history of malignancy (OR, 13.45; 95% CI, 8.36–21.64), and arterial hypertension (OR, 1.99; 95% CI, 1.9–2.1). Moreover, older patients exhibited a significantly higher likelihood of undergoing TLE due to infectious indications (OR, 4.36; 95% CI, 4.13–4.61) and were far less likely to have noninfectious indications (OR, 0.27; 95% CI, 0.26–0.28). Conversely, the patients below 80 years of age had significantly lower odds of having defibrillating devices (OR, 0.05; 95% CI, 0.05–0.06) and pacing devices (OR, 0.15; 95% CI, 0.14–0.16), as compared with the older cohort. The proportion of men was also higher in the older group (OR, 2.04; 95% CI, 1.94–2.14).
Authors | Country / region | Data | All patients, n | Patients <80 y, n | Patients ≥80 y, n | Mean (SD) age in patients <80 y | Mean (SD) age in patients ≥80 y | LE rate in patients <80 y, % | LE rate in patients ≥80 y, % | Pacing device in patients <80 y, n | Pacing device in patients ≥80 y, n | Defibrillating device in patients <80 y, n | Defibrillating device in patients ≥80 y, n |
Abbreviations: CRT‑P, cardiac resynchronization therapy pacemaker; CRT‑D, cardiac resynchronization therapy defibrillator; LE rate, lead extraction success rate; ND, not described; PM, pacemaker; others, see Table 1 | |||||||||||||
Akhtar et al16 | Six European centers | Retrospective (2005–2018) | 2052 | 1681 | 371 | <50 y: 37.7 (9.6) | 84.1 (3.7) | <50 y: 92.5 | 94.3 | ND | ND | ND | ND |
50–69 y: 61.4 (5.6) | 50–69 y: 94.6 | ||||||||||||
70–79 y: 75.9 (2.8) | 70–79 y: >94.8 | ||||||||||||
Al‑Maisary et al5 | Germany (Heidelberg University Hospital) | Retrospective (2013–2020) | 270 | 232 | 38 | 61 (14) | 83 (3) | 92.1 | 91.6 | ND | ND | ICD, 172 | ICD, 23 |
Burger et al15 | Germany (2 high‑volume centers) | Retrospective (2013–2017) | 71 | 0 | 71 | ND | 83.5 (3.3) | ND | 95.4 | ND | ND | ND | ND |
El‑Chami et al7 | USA (Emory University) | Retrospective (2007–2016) | 774 | 674 | 100 | 58.9 (14.6) | 84.7 (3.5) | 94.7 | 96 | ND | ND | ND | ND |
Giannotti et al20 | Italy (Pisa University Hospital) | Retrospective (2009–2018) | 1316 | 1114 | 202 | 66 (7) | 83 (2) | 96.4 | 98 | PM, 409; CRT‑P, 13 | PM, 122; CRT‑P, 13 | ICD, 704; CRT‑D, 313 | ICD, 79; CRT‑D, 54 |
Jachec et al19 | Poland and Italy (2 high‑volume centers) | Retrospective (2006–2017) | 3638 | 3089 | 549 | 64 (11.5) | 83 (2.5) | 95.1 | Octogenarians, 96.7 (n = 531) | 1735 | Octogenarians, 435 | 1297 | Octogenarians, 110 |
Nonagenarians, 97.1 (n = 34) | Nonagenarians, 30 | Nonagenarians, 5 | |||||||||||
Kempa et al22 | Poland (Medical University of Gdansk) | Retrospective (2003–2011) | 160 | 134 | 26 | 60.4 (14.3) | 83.7 (3.2) | 95.5 | 96.2 | ND | ND | ND | ND |
Kutarski et al31 | Poland (multiple centers) | Retrospective (2006–2013) | 1252 | 1060 | 192 | 62.7 (13.4) | 83.4 (3.1) | 94.6 | 97.4 | ND | ND | ND | ND |
Migliore et al21 | Italy (Padova and Bari, 2 centers) | Retrospective (2015–2022) | 83 | 0 | 83 | ND | 85 (3) | ND | 93.9 | ND | ND | ND | ND |
Okada et al32 | Japan (single‑center) | Retrospective (2014–2019) | 75 | 48 | 27 | 69.5 | 85 | 99 | 100 | 29 | 27 | 19 | 0 |
Pecha et al3 | Germany (GALLERY registry, 24 centers) | Retrospective (2013–2017) | 2524 | 2025 | 499 | 64.1 (12.4) | 84.3 (3.7) | 91.4 | 91.8 | 724 | 340 | 1303 | 160 |
Pelargonio et al14 | Italy and USA (multicenter) | Retrospective (2005–2011) | 849 | 699 | 150 | 61 (10) | 84 (3) | 96 | 97 | 385 | 126 | 314 | 24 |
Rodriguez et al23 | USA (University of Miami Hospital) | Retrospective (2004–2009) | 506 | 388 | 118 | 64.2 (12.4) | 85 (3.8) | 100 | 100 | 142 | 70 | 246 | 48 |
Williams et al6 | UK (St. Thomas’ Hospital, London) | Retrospective (2001–2011) | 406 | 334 | 72 | 62 (14.4) | 84 (3) | 98.5 | 98.6 | ND | ND | ND | ND |
Yagishita et al24 | Japan (Tokyo Medical and Dental University) | Retrospective (2013–2018) | 235 | 184 | 51 | ND | 86 (5) | 95.1 | 94.1 | 97 | 45 | 87 | 6 |
Ząbek et al27 | Poland (St. John Paul II Hospital, Kraków) | Prospective (2011–2019) | 667 | 577 | 90 | 64.2 (12.5) | 83.8 (2.8) | 96 | 97.8 | 346 | 73 | 231 | 17 |
Zhou et al28 | China (Shantou & Beijing, 2 centers) | Retrospective (2013–2021) | 1106 | 922 | 184 | 62 (13.7) | 83.8 (3.3) | 95.3 | 96.7 | 796 | 166 | 126 | 17 |
Variable | Patients <80 y (n = 11 396) | Patients ≥80 y (n = 14 880) | Odds ratio (95% CI) |
Men | 5875 | 10 180 | 2.04 (1.94–2.14) |
Pacing device | 4970 | 1527 | 0.15 (0.14–0.16) |
Defibrillating device | 5016 | 607 | 0.05 (0.05–0.06) |
Diabetes | 2069 | 4207 | 1.78 (1.67–1.89) |
Hypertension | 5087 | 9174 | 1.99 (1.9–2.1) |
Chronic renal failure | 919 | 3720 | 3.8 (3.52–4.1) |
History of malignancy | 18 | 310 | 13.45 (8.36–21.64) |
Coronary artery disease | 1210 | 4950 | 4.2 (3.92–4.49) |
Chronic obstructive pulmonary disease | 118 | 1108 | 7.69 (6.35–9.31) |
Infection | 5670 | 12 083 | 4.36 (4.13–4.61) |
Figure 1 presents the results of a meta‑analysis comparing the odds of complete procedural success. The analysis included 15 studies with a total of 15 830 patients (2669 aged ≥80 y and 13 161 aged <80 y), and showed OR of 1.26 (95% CI, 1.08–1.48), indicating that complete procedural success was significantly more likely in patients aged 80 years or older. No heterogeneity was observed across studies (I2 = 0%; τ2 = 0; P = 0.94).
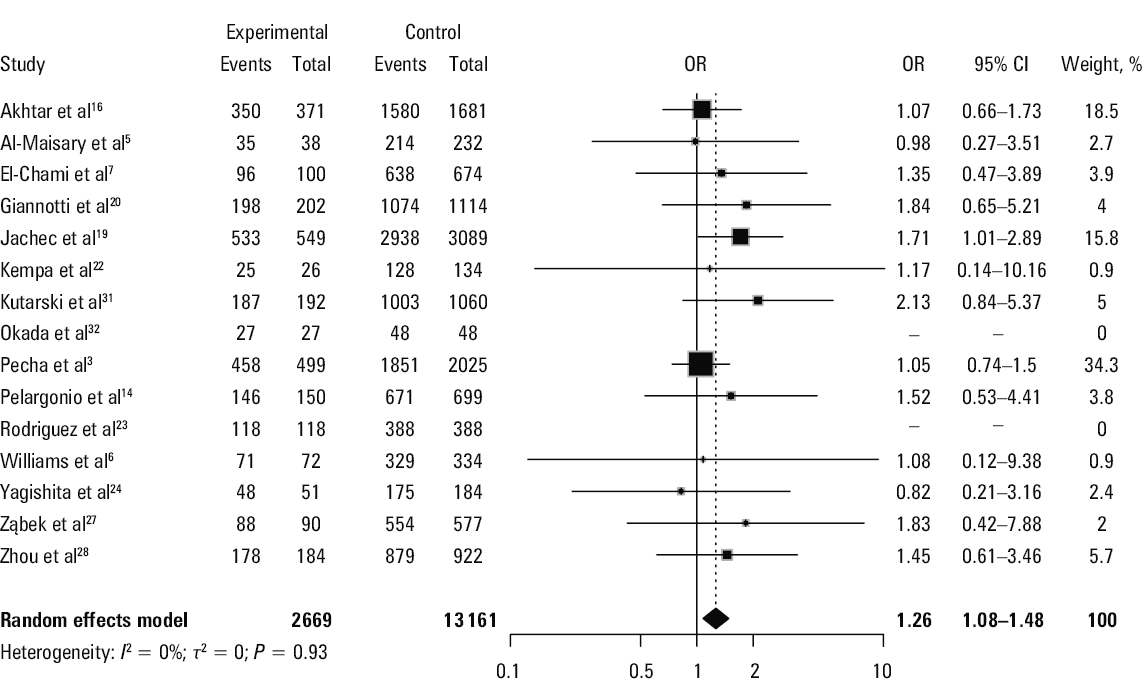
Abbreviations: OR, odds ratio
Figure 2A presents the results of a meta‑analysis comparing short‑term mortality following TLE. The analysis included 12 studies with a total of 14 148 patients (2413 aged ≥80 y and 11 735 aged <80 y), and yielded OR of 1.85 (95% CI, 1.56–2.2), thereby indicating a significantly higher risk of short‑term mortality in the patients aged at least 80 years. The absence of heterogeneity was observed across studies (I2 = 0%; τ2 = 0; P = 0.99).
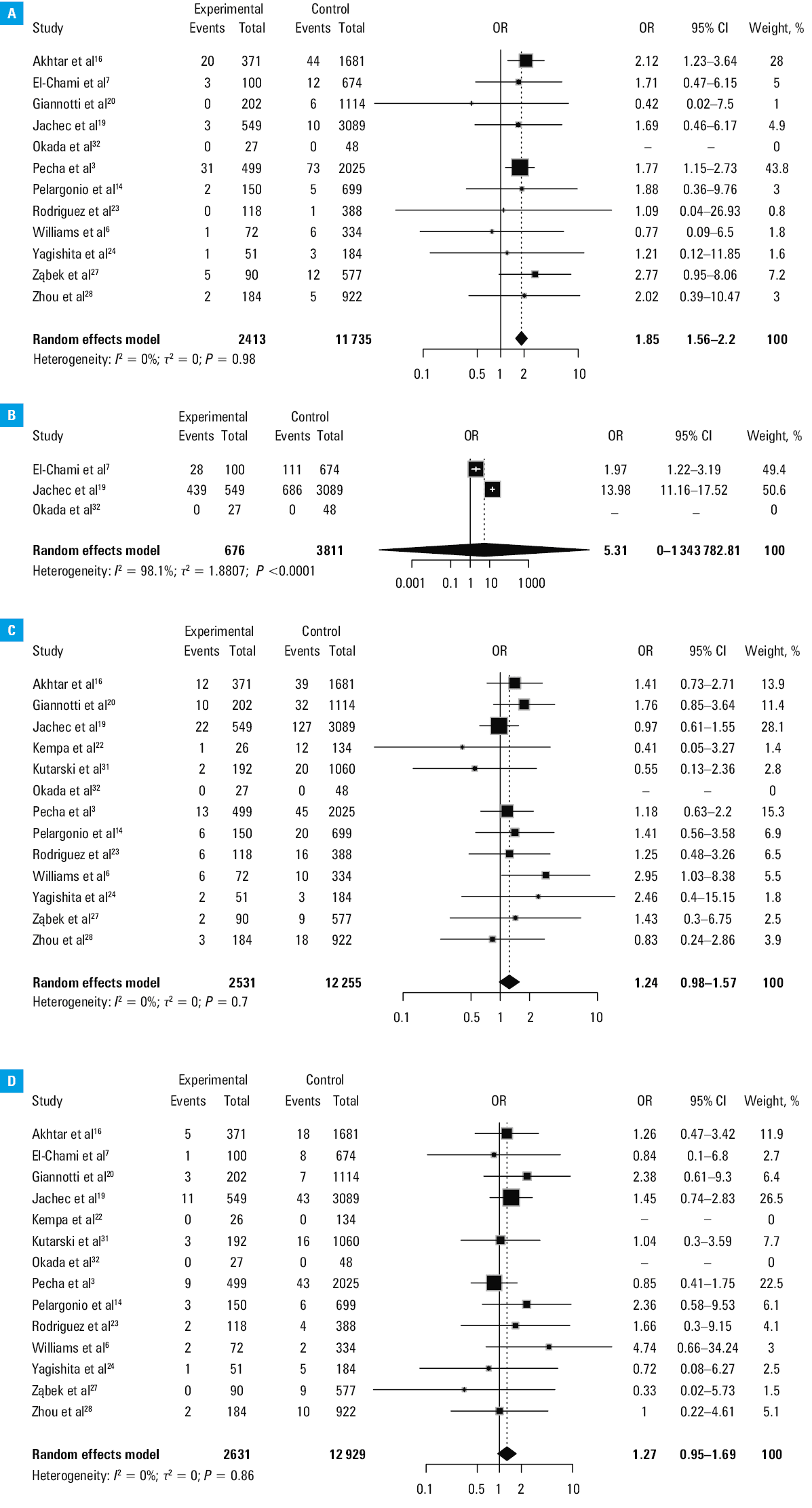
Abbreviations: see Figure 1
Figure 2B presents the results of a meta‑analysis comparing long‑term mortality following TLE. The analysis included 3 studies with a total of 4487 patients (676 aged ≥80 y and 3811 aged <80 y), and gave OR of 5.31 (95% CI, 0–1 343 782.81), reflecting extreme imprecision and suggesting inconclusive results. The analysis showed substantial heterogeneity (I2 = 98.1%; τ2 = 1.8807; P <0.001), indicating significant variability in study outcomes. Individual study weights were nearly equally distributed between 2 studies, while the third one had no weight due to 0 events.
Figure 2C presents the results of a meta‑analysis comparing the odds of minor complications following TLE. The analysis included 13 studies with a total of 14 786 patients (2531 aged ≥80 y and 12 255 aged <80 y), and the pooled OR was 1.24 (95% CI, 0.98–1.57), indicating no significant difference in the odds of minor complication between the age groups. Heterogeneity of the studies was not observed (I2 = 0%; τ2 = 0; P = 0.71), thereby supporting the consistency of results.
Figure 2D presents the results of a meta‑analysis comparing the incidence of major complications during TLE. The analysis included 13 studies, comprising a total of 15 920 patients (2631 aged ≥80 y and 12 929 aged <80 y), and the pooled OR was 1.27 (95% CI, 0.95–1.69), indicating no significant difference in the risk of major complications between the 2 age groups. No heterogeneity was observed among the included studies (I2 = 0%; τ2 = 0; P = 0.86).
Figure 3A presents the results of a meta‑analysis comparing the frequency of atrial lead removal. The analysis included 8 studies with a total of 6665 patients (1161 aged ≥80 y and 5504 aged <80 y), and yielded OR of 1.21 (95% CI, 0.9–1.63), indicating no significant difference between the age groups. Moderate heterogeneity was observed across studies (I2 = 58.6%; τ2 = 0.0681; P = 0.02), justifying the use of a random‑effects model.
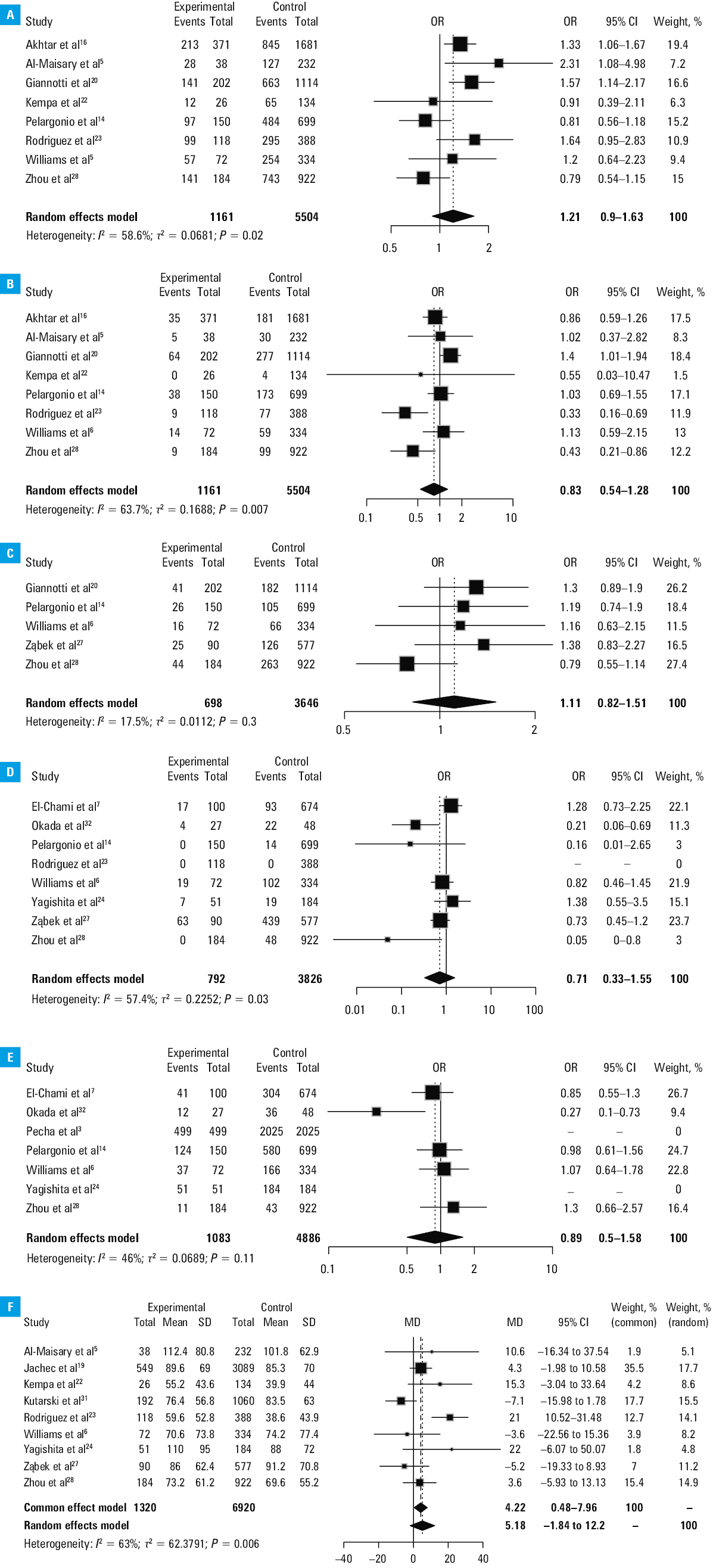
Abbreviations: MD, mean difference; others, see Figure 1
Figure 3B presents the results of a meta‑analysis comparing the frequency of coronary sinus lead removal. The analysis included 8 studies with a total of 6665 patients (1161 aged ≥80 y and 5504 aged <80 y), and yielded OR of 0.83 (95% CI, 0.54–1.28), indicating no significant difference between the age groups. Moderate heterogeneity was observed (I2 = 63.7%; τ2 = 0.1688; P = 0.007), supporting the choice of a random‑effects model.
Figure 3C presents the results of a meta‑analysis comparing the use of manual traction during lead extraction. The analysis included 5 studies with a total of 4362 patients (698 aged ≥80 y and 3646 aged <80 y), and yielded OR of 1.11 (95% CI, 0.82–1.51), indicating no significant difference between the age groups. Low heterogeneity was observed across studies (I2 = 17.5%; τ2 = 0.0112; P = 0.3), suggesting consistency in the findings.
Figure 3D presents the results of a meta‑analysis comparing the use of mechanical sheaths during lead extraction. The analysis included 8 studies with a total of 4618 patients (792 aged ≥80 y and 3826 aged <80 y), with pooled OR of 0.71 (95% CI, 0.33–1.55), indicating that here was no significant difference between the age groups. Moderate heterogeneity was observed across studies (I2 = 57.4%; τ2 = 0.2252; P = 0.03), supporting the use of a random‑effects model.
Figure 3E presents the results of a meta‑analysis comparing the use of laser sheaths during lead extraction. The analysis included 7 studies with a total of 5971 patients (1083 aged ≥80 y and 4886 aged <80 y), and yielded OR of 0.89 (95% CI, 0.5–1.58), indicating no significant difference between the age groups. Moderate heterogeneity was observed across studies (I2 = 46%; τ2 = 0.0689; P = 0.12).
Figure 3F presents the results of a meta‑analysis comparing the mean time from cardiac device implantation to extraction. The analysis included 8 studies comprising a total of 8240 patients (1320 aged ≥80 y and 6920 aged <80 y), and showed MD of 5.18 months (95% CI, –1.84 to 12.2), thereby indicating a nonsignificant trend toward a more protracted implantation duration among octogenarians. Substantial heterogeneity was observed across studies (I2 = 63%; τ2 = 62.38; P = 0.006), which justifies the use of a random‑effects model.
A summary of heterogeneity statistics and the Egger test for small‑study effects across key outcomes is presented in Supplementary material, Table S2 and Figures S2–S12.
Discussion
As the global population ages and the prevalence of CIEDs increases, understanding the risk‑benefit profile of TLE in octogenarians has become a critical aspect of cardiovascular care. The setting in which lead extraction is performed should be determined by the proper preoperative risk classification.25,26 Nevertheless, limited data in the available literature regarding the safety, efficacy, and TLE survival in octogenarians cause ambiguity and raise questions.4,5,19-23,27,28,31 Although TLE has been proven to be efficacious and safe in the general population, elderly patients are less often referred for this invasive procedure.28 A prevailing concern regarding increased periprocedural complication rates and higher long‑term mortality in octogenarians stems from the assumption that elderly patients are frailer and have more comorbidities.19,29 Although there is currently no official agreement on how elderly patients should be managed, Kennergren et al30 reported that the operators were often discouraged from performing TLE because of the patient advanced age.
In this systematic review and meta‑analysis, we included a total of almost 16 000 patients from 17 studies, providing the largest pooled evidence to date comparing TLE outcomes in patients aged at least 80 years and their younger counterparts. Noteworthy, the findings confirm that procedural success rates are comparable between the age groups, with complete lead extraction achieved in 94%–100% of the cases regardless of the patient age. Importantly, none of the analyzed studies demonstrated that TLE in elderly patients is associated with higher odds of major periprocedural complications or a reduced likelihood of procedural success. This observation directly challenges the perception that advanced age inherently increases the procedural risk.
A key aspect requiring clarification is the distinction between risk factors for procedure‑related complications and risk factors for long‑term mortality after lead removal. While octogenarians consistently demonstrated a higher burden of comorbidities, including CKD, CAD, COPD, and malignancy, these factors did not translate into increased odds of procedural complication. In‑hospital mortality remained low and comparable to that observed in younger cohorts across the included studies.
While the procedural success and safety were not inferior in octogenarians, our analysis identified significant differences in baseline characteristics and indications for TLE. Elderly patients were found more likely to undergo extraction due to infectious indications (OR, 4.36; 95% CI, 4.13–4.61), and less frequently for noninfectious causes (OR, 0.27; 95% CI, 0.26–0.28). These trends likely reflect both clinical necessity (eg, infection as a class I indication) and operator hesitancy toward nonurgent TLE in older, frailer patients. Furthermore, octogenarians had a higher burden of comorbidities, including CKD (OR, 3.8), CAD (OR, 4.2), COPD (OR, 7.69), and a markedly increased history of malignancy (OR, 13.45). Despite this, in‑hospital mortality remained low and comparable to that of younger patients in all of the included studies (OR, 1.85).
Another interesting finding is the distinct device profile across the age groups. The patients younger than 80 years were significantly more likely to have defibrillating devices (OR, 0.05), whereas pacing devices predominated in the above 80 years group. This device distribution is postulated to have a significant influence on periprocedural complexity and fluoroscopy time, particularly among younger patients undergoing ICD lead extraction.
The advanced age and presence of comorbidities were not linked to the safety and efficacy of TLE in octogenarians.14,28,31 There were no significant differences in the procedure duration in elderly and younger individuals, and the TLE in octogenarians was not associated with any additional technical issues.31 Additionally, in‑hospital mortality was particularly low in both octogenarians and younger populations.20,28,31 The key distinction was that the increased 30‑day all‑cause mortality in the individuals aged 80 years and older correlated with higher morbidity.27
These data confirm that advanced age alone should not preclude TLE, especially when clinically indicated. Nevertheless, it is imperative to apply individual risk‑benefit evaluation during determining the indication for TLE and planning the procedure. TLE should be performed exclusively by medical personnel fully capable of managing any unexpected or life‑threatening complications, and performing such additional procedures as sternotomy, thoracotomy, or cardiopulmonary bypass.19,32,33
Limitations
This study has several limitations that should be acknowledged. First, the majority of included studies were retrospective and single‑center, which may introduce selection bias and limit generalizability. The data regarding frailty indices, cognitive status, or functional capacity—important variables in decision‑making in elderly patients—were not consistently reported, precluding a detailed risk stratification beyond chronological age.
Second, despite the substantial cumulative sample size, heterogeneity in reporting and data completeness (eg, device type breakdowns, cause‑specific mortality, procedural details) limited the possibility of deeper subgroup analysis. In particular, the definition of complications and procedural success varied slightly across studies, despite the adherence to the established international clinical practice guidelines. As a result, heterogeneity among the included studies partially diminished the reliability of the pooled effect estimate and limited the ability to draw broadly generalizable conclusions.
Third, while the Egger test for publication bias did not indicate significant asymmetry in most outcomes, the number of studies included per outcome was sometimes limited, decreasing the power of such assessments.
Fourth, the long‑term outcomes beyond 30 days were reported inconsistently, and were not available in sufficient detail for the pooled analysis. This restricted our ability to assess the prognostic effect of TLE on survival and quality of life in octogenarians.
The overall judgment of evidence quality may be regarded as moderately high, supported by strong source reliability, sound methodology, and substantial relevance, although limitations in transparency and reproducibility constrain its robustness.
Finally, although the age of 80 years was used as a threshold, individual variation in biological age and frailty may be more relevant than age alone. Further prospective, multicenter studies using frailty‑adjusted and indication‑specific models are warranted to refine clinical decision‑making for TLE in the elderly.
Conclusions
Despite higher prevalence of comorbidities and predominance of infectious indications in the elderly population, procedural outcomes of TLE did not differ significantly between the age groups. Importantly, short‑term mortality was slightly increased in octogenarians, likely reflecting underlying frailty and clinical complexity rather than procedural failure.
The findings of this study support the notion that advanced age alone should not be considered a contraindication to TLE. Instead, a comprehensive, individualized approach considering the indication, comorbidity burden, and procedural setting is warranted. Further prospective, multicenter studies are needed to refine risk stratification and optimize outcomes in this growing patient population.
- Kitzman DW, Whellan DJ, Duncan P, et al. Physical rehabilitation for older patients hospitalized for heart failure. N Engl J Med. 2021; 385: 203‑216. | Crossref
- Wang Y, Xiao Y, Tang J, et al. Effects of early phase 1 cardiac rehabilitation on cardiac function evaluated by impedance cardiography in patients with coronary heart disease and acute heart failure. Front Cardiovasc Med. 2022; 9: 1‑10. | Crossref
- Pecha S, Chung DU, Burger H, et al. Laser lead extraction in octo- and nonagenarians: a subgroup analysis from the GALLERY registry. J Cardiovasc Electrophysiol. 2023; 34: 1951‑1960. | Crossref
- Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021; 42: 3427‑3520. | Crossref
- Al‑Maisary S, Romano G, Karck M, et al. Octogenarian patients and laser‑assisted lead extraction: should we put a limit? PLoS One. 2023; 18: 1‑8. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION