Clinical utility of symptom-based assessment as an indicator of objective gastroesophageal reflux disease
Key words: ambulatory reflux monitoring, gastroesophageal reflux disease, Lyon Consensus, pH-impedance

 CC BY 4.0
CC BY 4.0
Clinical utility of symptom-based assessment as an indicator of objective gastroesophageal reflux disease
Introduction: Patients with troublesome reflux‑like symptoms, in whom routine empirical proton pump inhibitor (PPI) therapy is often unsatisfactory, present a therapeutic challenge and are frequently referred for gastroenterological evaluation to confirm a diagnosis of gastroesophageal reflux disease (GERD).
Objectives: We aimed to determine the prevalence of objectively confirmed GERD (diagnosed according to the Lyon Consensus 2.0 criteria) in patients with typical and / or atypical troublesome reflux‑like symptoms who did not respond or partially responded to PPI therapy, and were referred for esophageal pH‑impedance monitoring.
Patients and methods: This was a retrospective study analyzing pH‑impedance monitoring results of 500 patients who previously underwent endoscopy. A conclusive GERD diagnosis was defined as an acid exposure time (AET) greater than 6%, or 4%–6% with supporting evidence (number of reflux episodes >80/d, and / or mean nocturnal basal impedance <1500 Ω, and / or a positive reflux–symptom association).
Results: Of the 500 patients analyzed, 477 reported symptoms, which were categorized as follows: isolated typical (n = 49; 10.3%), both typical and atypical (n = 206; 43.2%), and isolated atypical (n = 222; 46.5%). AET greater than 6% was found in 12 (24.5%), 41 (19.9%), and 27 patients (12.2%) in each group, respectively. The inclusion of supportive evidence for patients with AET of 4%–6% increased the number of GERD diagnoses in each group to 23 (46.9%), 68 (33%), and 40 (18%), respectively. When endoscopy findings were factored in, the prevalence of GERD in the whole study population increased from 27% (n = 135) to 29.6% (n = 148). Among the 161 individuals reporting heartburn, 41.6% met the criteria of functional heartburn.
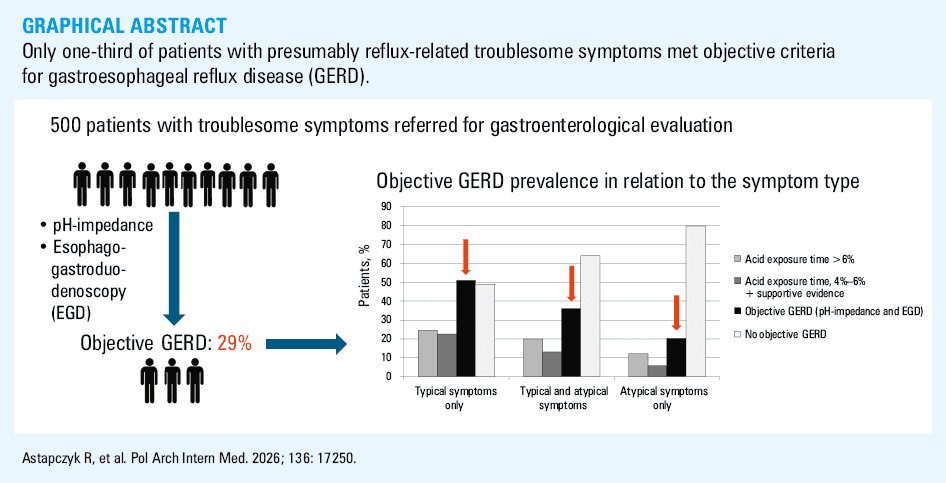
Conclusions: Only 29.6% of the patients referred for GERD evaluation fulfilled the objective diagnostic criteria for the disease. GERD was present in about half of the patients with isolated typical symptoms, one‑third of those with both typical and atypical symptoms, and fewer than one‑fifth of those with isolated atypical symptoms.
What's new?
In clinical practice, symptoms suggestive of gastroesophageal reflux disease (GERD) represent one of the most common gastrointestinal complaints, and are routinely treated with proton pump inhibitors (PPIs). This study assessed the clinical utility of symptom‑based evaluation as a primary indicator of GERD. Among patients with troublesome, presumably reflux‑related symptoms referred for gastroenterological assessment, only one‑third fulfilled objective diagnostic criteria for GERD. Specifically, GERD was confirmed in approximately half of the patients reporting typical symptoms alone, and in one‑third of those presenting with both typical and atypical symptoms. The high prevalence of functional heartburn among the patients with typical symptoms underscores the importance of objective GERD confirmation through reflux monitoring before initiating long‑term PPI therapy. Conversely, fewer than one‑fifth of the patients with isolated atypical symptoms demonstrated objective evidence of GERD, supporting current recommendations against routine empirical PPI therapy in this subgroup.
Introduction
Gastroesophageal reflux disease (GERD) is commonly diagnosed in outpatient practice.1-3 According to the Montreal Consensus,1 GERD develops when the reflux of stomach contents into the esophagus causes troublesome symptoms (ones that adversely affect patient well‑being or quality of life) and / or complications.1 A wide range of typical (eg, heartburn, regurgitation) and atypical (eg, pulmonary and laryngeal manifestations) symptoms have been associated with GERD.1,4,5 For patients with typical manifestations who have no alarm symptoms, empirical treatment with a proton pump inhibitor (PPI) is recommended.4 However, thorough evaluation before starting PPI therapy is advised in individuals with extraesophageal manifestations without concomitant typical symptoms.4 GERD should be objectively documented in the cases of diagnostic uncertainty or treatment failure, or in the patients who are referred for long‑term medical therapy or surgical treatment.5 Recently, the Lyon Consensus 2.0 introduced criteria for a modern diagnosis of GERD to improve its diagnostic specificity and confidence.5 According to these criteria, objective endoscopic findings of GERD include erosive esophagitis of a Los Angeles grade B or higher, Barrett esophagus, and peptic stricture. On reflux monitoring, total acid exposure time (AET) greater than 6% is diagnostic of GERD, while AET of 4%–6% is inconclusive. Adjunctive evidence for pathological reflux includes a total number of reflux episodes exceeding 80/day, a positive reflux–symptom association, and mean nocturnal baseline impedance (MNBI) lower than 1500 Ω.5
Individuals presenting with troublesome symptoms that are considered to be GERD‑related and negatively impact quality of life pose a diagnostic and therapeutic challenge in outpatient practice, as it is uncertain whether they should be treated as true GERD patients. Most of these patients have a history of at least 1 esophagogastroduodenoscopy (EGD) examination without findings indicative of reflux, such as erosive esophagitis or Barrett esophagus. Furthermore, 20%–40% of individuals with heartburn do not respond to PPIs.6,7 An overlap between GERD and functional disorders complicates management of such patients.8,9 Additionally, extraesophageal manifestations, even isolated ones, are frequently believed to be caused by GERD based on symptom evaluation and / or laryngeal findings, resulting in frequent and often unnecessary PPI prescriptions.4,5 Consequently, such patients are often referred for gastroenterological evaluation to confirm the GERD diagnosis.
In this large, real‑world, retrospective study, we assessed the prevalence of objectively confirmed GERD (based on the new Lyon Consensus 2.0 criteria5) among patients with troublesome typical and / or atypical reflux symptoms referred for pH‑impedance monitoring.
Patients and methods
Patients
We retrospectively evaluated ambulatory 24‑hour esophageal pH and impedance monitoring tracings of 500 consecutive adult patients with troublesome symptoms referred for reflux testing. The patients reported typical symptoms, such as heartburn and regurgitation, and / or atypical symptoms, including cough, chest pain, belching, abdominal pain, and laryngeal symptoms (hoarseness, globus, postnasal drip, bitter taste, throat pain, throat clearing). All patients with atypical / extraesophageal symptoms were evaluated by other specialists (eg, cardiologists, laryngologists, or pulmonologists) before referral for testing, and non‑GERD causes were excluded. In addition, all patients were treated with PPIs with no or partial response to treatment, and previously underwent EGD. The pH‑impedance monitoring was performed off PPI therapy to confirm or rule out a GERD diagnosis (details presented in Supplementary material). Prior to reflux monitoring, high‑resolution manometry was performed to locate the lower esophageal sphincter and exclude major motility disorders.
All participants gave their written informed consent before undergoing any procedures. The patients were not exposed to any additional interventions for the purpose of this study. The ethical committee review was deemed unnecessary due to the retrospective nature of the study.
Twenty‑four–hour esophageal pH‑impedance monitoring
The following parameters were evaluated: AET (total; in upright and recumbent positions), number of reflux episodes (total; in upright and recumbent positions; proximal), MNBI, number of symptoms, and reflux–symptom association, assessed using a symptom index (SI) score and symptom association probability (SAP). The patients were classified based on AET values: below 4% (normal), between 4% and 6% (inconclusive), and greater than 6% (abnormal). The total number of reflux episodes exceeding 80/day was considered abnormal, 40–80 episodes/day were deemed inconclusive, and less than 40 episodes/day were considered normal. The respective normal, inconclusive, and abnormal MNBI ranges were greater than 2500 Ω, 1500–2500 Ω, and below 1500 Ω. A positive reflux–symptom association was found with an SI greater than 50% and SAP greater than 95%. Based on the Lyon Consensus 2.0 criteria,5 a conclusive GERD diagnosis was confirmed when AET was greater than 6%. Pathological reflux was excluded with AET values below 4%. In the cases of an inconclusive AET value (4%–6%), presence of further supportive GERD evidence was considered (total number of reflux episodes >80/d, and / or MNBI <1500 Ω, and / or a positive reflux–symptom association).5
All troublesome symptoms reported by the patients were analyzed. A separate analysis of specific symptoms (eg, heartburn, regurgitation, laryngopharyngeal manifestations, cough) was also performed. We assessed the relationship between the reported symptom type and pH‑impedance parameters, and a conclusive GERD diagnosis based on the Lyon Consensus 2.0 criteria.
Statistical analysis
Statistical analysis was performed using R software (version 4.1.2; R Foundation for Statistical Computing, Vienna, Austria). Quantitative variables are presented as mean and SD or median and interquartile range, depending on their distribution. Categorical variables are described as number (percentage). Distribution normality was checked with the Shapiro–Wilk test and verified with skewness and kurtosis (normality was assumed when the skewness and kurtosis values were between –2 and 2). The Levene test was used to analyze variance homogeneity. Comparison of quantitative variables was performed with the analysis of variance, Kruskal–Wallis test, t test, or Mann–Whitney test, as appropriate. Categorical variables were compared with the Pearson χ2 test or Fisher exact test, as applicable. The Dunn test with Bonferroni adjustment was used for pairwise comparisons in the cases of significant Kruskal–Wallis test outcomes. The Benjamini–Hochberg adjustment was used for pairwise comparisons of categorical variables. Univariable logistic regression analysis was performed to identify the predictors of a positive reflux–symptom association. Subsequently, a multivariable logistic regression model was built, including all variables that were significant in the univariable analysis. A P value below 0.05 was considered significant.
Results
Patients characteristics
The pH‑impedance monitoring tracings from 500 patients (316 women, 184 men) were analyzed. The patients were monitored off PPI therapy, which was stopped at least 7 days before the examination. Overall, 477 individuals (95.4%) reported symptoms during reflux monitoring. A total of 161 patients (33.8%) reported heartburn, and 146 (30.6%) had regurgitation. The following atypical symptoms were reported: belching (n = 275; 57.7%), laryngopharyngeal symptoms (n = 139; 29.1%), abdominal pain (n = 153; 32.1%), cough (n = 86; 18.1%), chest pain (n = 49; 10.3%), and dysphagia (n = 19; 4%). The most common laryngopharyngeal symptoms were globus (n = 47), throat pain (n = 36), postnasal drip (n = 25), bitter taste (n = 24), hoarseness (n = 20), and throat clearing (n = 14).
The study population was divided into 3 groups based on the main type of reported symptoms: patients with typical symptoms only (n = 49; 10.3%), patients with both typical and atypical symptoms (n = 206; 43.2%), and patients with atypical symptoms only (n = 222; 46.5%). The groups did not differ in terms of sex distribution or mean age, although the median body weight was the highest in the patients reporting isolated typical symptoms (Supplementary material, Table S1).
pH‑impedance parameters
A summary of pH and impedance monitoring parameters according to the type of symptoms reported by the patients is presented in Table 1. The patients with isolated atypical symptoms had lower AET, fewer reflux episodes, and higher MNBI values than those reporting typical symptoms alone. The median number of reported symptoms was higher in the patients with both typical and atypical symptoms than in the individuals with either typical or atypical symptoms occurring in isolation (Table 1).
Parameter | Patients with isolated typical symptoms (n = 49) | Patients with typical and atypical symptoms (n = 206) | Patients with isolated atypical symptoms (n = 222) | P value | |
Data are presented as median (interquartile range).
a Significant difference (P <0.05) between the patients with isolated typical vs isolated atypical symptoms
b Significant difference (P <0.05) between the patients with isolated atypical vs both typical and atypical symptoms
c Significant difference (P <0.05) between the patients with isolated typical vs both typical and atypical symptoms | |||||
Acid exposure time, % | Total | 3.8 (1.4–5.5)a | 1.8 (0.4–5) | 1.2 (0.3–3.58)a | 0.001 |
Upright position | 5.7 (1–7.9)a | 2.8 (0.5–7.5)b | 1.7 (0.4–4.38)a,b | 0.003 | |
Recumbent position | 0.3 (0–2.6)a | 0.2 (0–1.98) | 0.1 (0–1)a | 0.04 | |
Reflux episodes/day, n | Total | 60 (42–88)a | 57.5 (35–90.5)b | 46 (30–70)a,b | 0.003 |
Upright position | 49 (33–69) | 50 (31–76)b | 41 (27–58)b | 0.003 | |
Recumbent position | 8 (2–17) | 6 (2–4) | 4 (31–76) | 0.11 | |
Acid | 38 (14–59)a | 27 (11–56)c | 21 (9–36)a,b | <0.001 | |
Nonacid | 22 (15–34) | 23.5 (12–38) | 21.5 (13–37.75) | 0.96 | |
Proximal | 27.5 (16.75–38.75) | 30 (15–47)b | 21 (10.75–34.25)b | 0.001 | |
Mean nocturnal baseline impedance, Ω | 1893 (1469–2567)a | 2292 (1500–2671)b | 2671 (2102–2923)a,b | <0.001 | |
Symptoms, n | 3.5 (2–8.75)c | 11 (5–25)b,c | 5.5 (2–20)b | 0.001 | |
A total of 23 patients (4.6%) did not record any symptoms during 24‑hour reflux monitoring. There were no significant differences in median AET values, number of reflux episodes, or MNBI between the patients who did and those who did not record the symptoms during monitoring (Supplementary material, Table S2).
In an additional analysis, we assessed the distribution of abnormal, inconclusive, and normal AET values in the whole study population, regardless of the type of symptoms reported. Among the 500 patients analyzed, 353 (70.3%) had AET below 4%, 64 (12.8%) had AET between 4% and 6%, and 83 (16.6%) had AET exceeding 6%. The patients with AET greater than 6% had significantly higher median body weight and a higher total number of reflux episodes than the individuals with AET below 4% (Supplementary material, Table S3). MBNI, as an additional parameter included in the Lyon Consensus 2.0,5 correlated negatively with AET (total; in upright and recumbent positions) and the number of reflux episodes (total, acid; Supplementary material, Table S4). The median MNBI values were significantly lower in the patients with AET above 6% than in those with AET of 4%–6% or below 4%. Moreover, the individuals with inconclusive AET values (4%–6%) had lower MNBI than those with normal AET (<4%; Supplementary material, Table S3).
Distribution of normal, inconclusive, and abnormal values of acid exposure time by symptom type
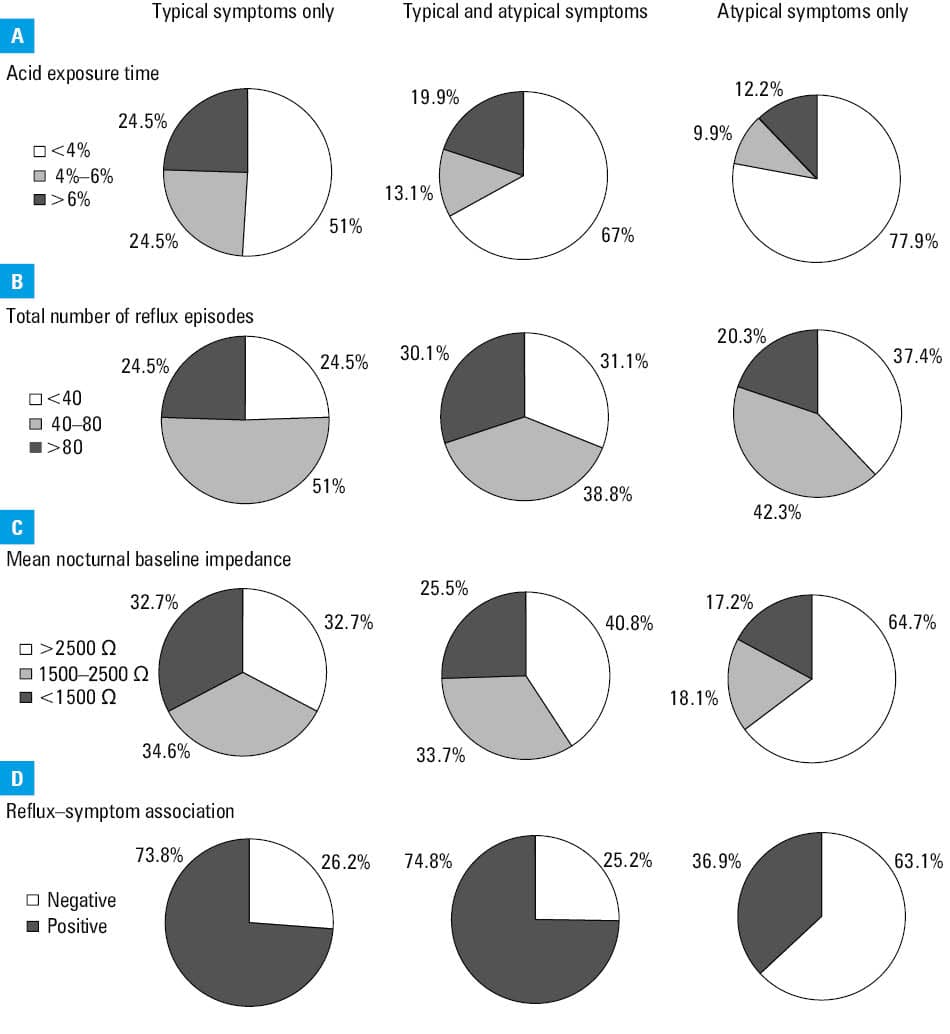
The presence of atypical symptoms increased the probability of detecting normal AET values. AET below 4% was found in 78% of the patients with isolated atypical symptoms, 67% of those with both typical and atypical symptoms, and 51% of the participants with typical symptoms only. In contrast, the prevalence of AET greater than 6% was lower in the patients with isolated atypical symptoms. There were no significant differences between the patients reporting typical symptoms alone and those with both typical and atypical symptoms (Figure 1A; Supplementary material, Table S5).
Distribution of normal, inconclusive, and abnormal total number of reflux episodes by symptom type
The distribution of the total number of reflux episodes in relation to the type of symptoms reported was similar across the groups, except for the prevalence of the abnormal number of reflux episodes (>80), which was higher in the patients with both typical and atypical symptoms than in those with atypical symptoms only (Figure 1B; Supplementary material, Table S5)
Distribution of normal, inconclusive, and abnormal mean nocturnal baseline impedance values by symptom type
Prevalence of MNBI values greater than 1500 Ω was significantly higher in the patients reporting atypical symptoms alone than in those with isolated typical symptoms or both typical and atypical symptoms (Figure 1C; Supplementary material, Table S5).
Distribution of positive and negative reflux–symptom association by symptom type
About 63% of the patients with isolated atypical symptoms had a negative reflux–symptom association expressed by negative SI and SAP indices, while more than 73% of the patients with typical symptoms had a positive reflux–symptom association (Figure 1D; Supplementary material, Table S5).
Objective gastroesophageal reflux disease findings based on the Lyon Consensus 2.0 criteria
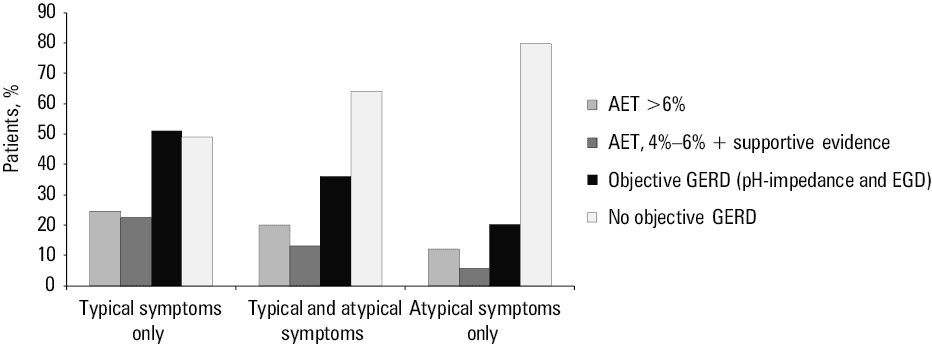
Among the 12 patients (24.5%) with isolated typical symptoms and inconclusive AET values, 11 had supportive evidence of pathological reflux. This increased the diagnostic rate of conclusive GERD from 24.5% (12 patients with AET >6%) to 46.9% (23 patients; Figure 2).
Abbreviations: AET, acid exposure time; EGD, esophagogastroduodenoscopy; GERD, gastroesophageal reflux disease
Among the patients with both typical and atypical symptoms, inconclusive AET values were present in 27 individuals (13.1%), all of whom had supportive evidence for pathological reflux. Thus, the rate of conclusive GERD diagnosis increased from 19.9% (n = 41) to 33% (n = 68; Figure 2).
Inconclusive AET values were observed in 22 patients (9.9%) with isolated atypical symptoms, of whom 13 (59.1%) had supportive evidence of pathological reflux (all with MNBI <1500 Ω and / or >80 reflux episodes/d; 8 patients also had a positive reflux–symptom association). Therefore, the diagnostic rate of conclusive GERD increased from 12.2% (27 patients with AET >6%) to 18% (40 patients; Figure 2).
The results of EGD were available for 460 patients (92%). Of those, 83.7% had no endoscopic evidence of reflux. The analysis of EGD findings identified 13 additional patients with conclusive evidence for pathological reflux (erosive esophagitis stage B according to the Los Angeles classification) who had inconclusive values of pH and impedance monitoring parameters, including 2 patients with typical symptoms, 6 with both typical and atypical symptoms, and 5 with isolated atypical symptoms. Taking into account the results of pH‑impedance monitoring and EGD, a diagnosis of objective GERD was made in 25 (51%), 74 (35.9%), and 45 (20.3%) of the patients with isolated typical, both typical and atypical, and isolated atypical symptoms, respectively (Figure 3). Consequently, in the patients who reported symptoms during monitoring, the rate of objective GERD diagnosis increased from 27.5% (n = 131) to 30.2% (n = 144). The presence of isolated atypical symptoms was associated with a significantly lower prevalence of objective GERD. Overall, the diagnostic rate of objective GERD in the whole study population (n = 500; including 4 patients with conclusive GERD who did not report symptoms during pH and impedance monitoring) increased from 27% to 29.6% (n = 148).
Interestingly, using older criteria for abnormal AET (>4.2%),10 pathological reflux was diagnosed in 46.9%, 33%, and 21.6% of the patients with isolated typical, both typical and atypical, and isolated atypical symptoms, respectively.
Individual symptoms and reflux–symptom association indices
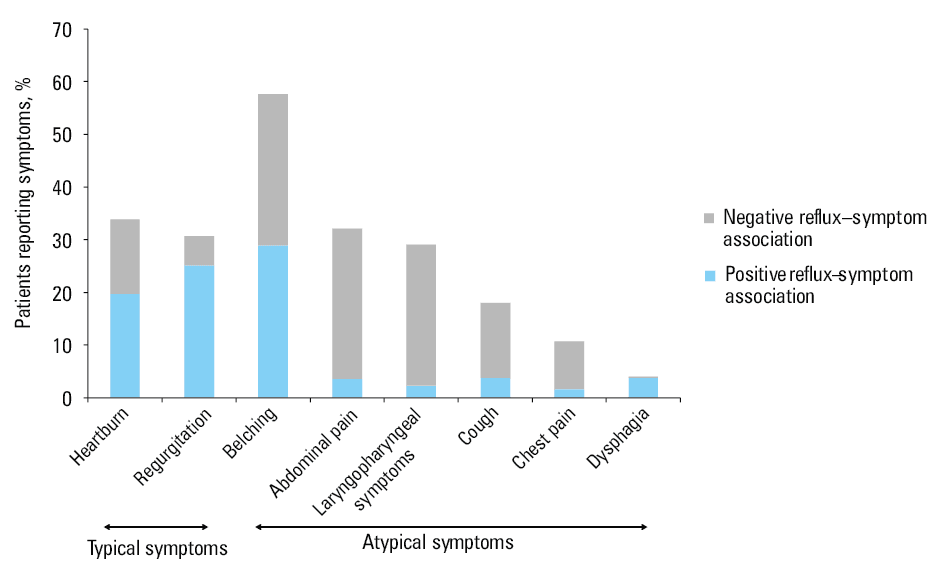
The percentage of all study patients reporting individual symptoms, and the association of each symptom with reflux based on reflux–symptom indices (SI and SAP) assessed by pH‑impedance monitoring are shown in Figure 3. Heartburn and regurgitation were reported by approximately one‑third of all study patients, and showed a positive association with reflux in 58.4% (n = 94 of 161) and 82.2% (n = 120 of 146).
Among the atypical symptoms, belching was positively associated with reflux in about half of all patients. The remaining atypical symptoms rarely showed a positive association with reflux (Figure 3). However, the frequency of each individual symptom occurrence was similar between the study groups (Table 2). Specifically, except for belching, all other atypical symptoms (eg, laryngopharyngeal symptoms) occurred with a similar frequency in the patients with both typical and atypical symptoms and those with atypical symptoms alone. Furthermore, their positive reflux–symptom association was likewise unrelated to the presence of concomitant typical symptoms (Table 2). The frequency of individual symptoms in relation to the AET values is described in Supplementary material, Table S6.
Parameter | Patients with isolated typical symptoms (n = 49) | Patients with typical and atypical symptoms (n = 206) | Patients with isolated atypical symptoms (n = 222) | P value | |
Data are presented as number (percentage).
a SAP ≥95% and SI ≥50% were considered indicative of a positive reflux–symptom association.
b The percentages of patients with positive SI/SAP were calculated in relation to the number of patients reporting a given symptom.
Abbreviations: SAP, symptom association probability; SI, symptom index | |||||
Heartburn | Overall prevalence | 34 (69.4) | 127 (61.7) | – | 0.4 |
Positive SI/SAPa,b | 16 (47.1) | 78 (61.4) | – | 0.17 | |
Regurgitation | Overall prevalence | 22 (44.9) | 124 (60.2) | – | 0.052 |
Positive SI/SAP | 22 (100) | 98 (80.3) | – | 0.11 | |
Belching | Overall prevalence | – | 121 (58.7) | 154 (69.4) | 0.04 |
Positive SI/SAP | – | 62 (51.2) | 76 (49.4) | 0.89 | |
Abdominal pain | Overall prevalence | – | 79 (38.4) | 74 (33.3) | 0.33 |
Positive SI/SAP | – | 9 (11.4) | 8 (10.8) | >0.99 | |
Laryngopharyngeal symptoms | Overall prevalence | – | 68 (33) | 71 (32) | 0.9 |
Positive SI/SAP | – | 6 (8.8) | 5 (7) | 0.81 | |
Cough | Overall prevalence | – | 44 (21.4) | 39 (17.6) | 0.39 |
Positive SI/SAP | – | 1 (10) | 0 | – | |
Chest pain | Overall prevalence | – | 28 (13.6) | 21 (9.5) | 0.23 |
Positive SI/SAP | – | 3 (10.7) | 2 (9.5) | >0.99 | |
Dysphagia | Overall prevalence | – | 10 (4.9) | 9 (4.1) | 0.3 |
Positive SI/SAP | – | 1 (10) | 0 | – | |
Next, we analyzed factors correlating with a positive reflux–symptom association. In univariable logistic regression analysis, the factors significantly correlated with a positive reflux–symptom association were regurgitation, heartburn, ACT (total; in upright and recumbent positions), number of reflux episodes (total; in upright and recumbent positions), number of acid reflux episodes, number of nonacid reflux episodes, MNBI, belching, and a lack of laryngopharyngeal symptoms. However, in multivariable logistic regression analysis, only regurgitation, belching, and number of reflux episodes in the upright position were predictive of a positive reflux–symptoms association (Supplementary material, Table S7).
Typical symptoms negatively associated with reflux
Among the 161 patients with heartburn, 100 (62.1%) had normal AET, 27 (16.8%) had inconclusive AET, and 34 (21.1%) had abnormal AET. In 59 individuals with normal AET, heartburn showed no association with reflux. In contrast, heartburn was unrelated to reflux in 13% (n = 8 of 61) of the patients with inconclusive and abnormal AET (Figure 4). Overall, 41.6% (n = 67 of 161) of the patients with heartburn met the criteria for functional heartburn.
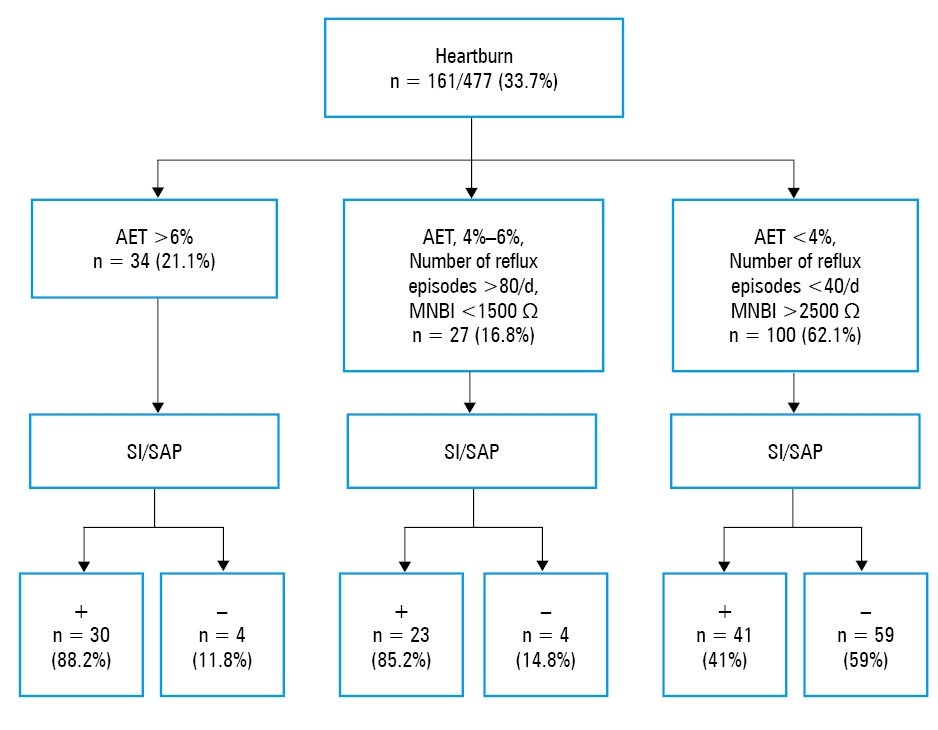
Abbreviations: MNBI, mean nocturnal baseline impedance; others, see Table 2 and Figure 2
Among the 146 patients with regurgitation, normal AET was detected in 97 individuals (66.4%), inconclusive AET in 20 (13.7%), and abnormal AET in 29 (19.9%). In 23 patients with normal AET (23.7%), regurgitation showed no association with reflux.
Discussion
In this large, real‑world study, we investigated the rate of objective GERD diagnoses in patients presenting with troublesome typical and atypical reflux symptoms. The prevalence of GERD in European countries has been estimated at between 9% and 26%, but in patients presenting with troublesome symptoms, particularly extraesophageal ones, it varies according to factors such as selection bias, study population, and applied methodology.3 In our study, GERD was ultimately diagnosed in approximately 29% of the patients based on the Lyon Consensus 2.0 criteria.5 In line with previous research, we found that pathological reflux was associated with an increased body weight, but not with sex or age.3,4,11,12 Although the retrospective design is the main limitation of our study, it remains one of the largest analyses evaluating objective GERD in consecutive patients referred for esophageal testing to determine whether their troublesome, PPI‑refractory symptoms were truly related to GERD. The study group represents a patient population of the north‑eastern part of Poland, referred by specialists for further gastroenterological evaluation. Notably, patients with isolated typical symptoms were rarely referred, accounting for only 10% of this cohort. Indeed, atypical manifestations present challenges for both patients and physicians, and are often the main indication for further testing.
When analyzing pH‑impedance monitoring parameters, total AET greater than 6% while off PPI therapy is diagnostic of GERD, and has been considered as the most reproducible parameter identifying patients who are likely to respond to medical or surgical treatments.4,5 AET of 4%–6% is deemed inconclusive, whereas AET below 4% excludes pathological reflux.4 In this study, 16.6% of all patients with troublesome symptoms had AET exceeding 6%, whereas 12.8% had inconclusive AET values. The inclusion of adjunctive evidence for pathological reflux on pH‑impedance monitoring increased the final rate of GERD diagnosis to 26.2%. In a retrospective study of 249 Greek patients, 25% of the patients had conclusive GERD based on the 2018 Lyon Consensus criteria.13 In an Italian study, 23% and 17% of 317 patients exhibited abnormal and inconclusive AET values, respectively. When abnormal impedance metrics were considered in the cases with inconclusive AET values, the rate of GERD diagnosis increased from 23% to 37%.14 However, the patient populations differed between these studies. In the Greek study, 56.2% of the patients had typical symptoms and 39.6% presented with extraesophageal symptoms. The presence of typical symptoms correlated with GERD diagnosis, but a more detailed symptom analysis was not performed.13 The Italian study included only patients with heartburn refractory to PPI therapy.14 Our study focused on evaluating reflux metrics according to the type of troublesome symptoms in consecutive patients referred for testing following an unsatisfactory response to PPIs. Of those, nearly half exhibited typical symptoms alone or in combination with atypical ones, whereas the remaining had isolated atypical symptoms.
As expected, the presence of typical symptoms was associated with a significantly higher acid burden, as compared with isolated atypical symptoms. AET values greater than 6% were nearly twice as common in the patients with typical symptoms (with or without atypical symptoms) as in those with isolated atypical symptoms. When adjunctive parameters were analyzed in the patients with inconclusive AET values, the rate of GERD diagnosis increased up to approximately half of the patients with typical symptoms only, and to one‑third of those with both typical and atypical symptoms. This suggests that the greatest diagnostic value lies in identifying conclusive or inconclusive AET values in the patients with typical symptoms, as adjunctive parameters supporting the diagnosis are present in almost all cases with inconclusive AET. Similarly, Jiang et al15 reported that patients with typical symptoms and inconclusive AET had significantly more positive adjunctive evidence of GERD.
In contrast, the presence of isolated atypical symptoms appears to reduce the likelihood of objective GERD diagnosis, as only 12.2% of such patients had AET above 6%, and adjunctive parameters in the inconclusive cases increased the diagnostic rate by just 6%. In a study of 50 patients with laryngeal symptoms and laryngoscopic findings suggestive of reflux, 14% had elevated AET, while prolonged bolus exposure time and / or an increased number of reflux episodes, despite normal AET values, provided an additional diagnostic yield of 18%.16 In another study, 17% of the patients with chronic cough had AET greater than 5%, but half of these patients also reported typical symptoms.17 Calabrese et al18 applied the Lyon Consensus 2.0 criteria in the evaluation of extraesophageal symptoms, either isolated or accompanied by typical ones. GERD was confirmed in 29.2% of 274 patients, including 41 with AET greater than 6% and 39 with AET of 4%–6% supported by adjunctive evidence. However, the prevalence of concomitant atypical and typical symptoms did not differ between the patients with and without GERD.18
According to the Lyon Consensus 2.0 criteria, the assessment of adjunctive GERD parameters, such as reflux–symptom association evaluated by SI and SAP indices, MNBI, and the number of reflux episodes, is recommended in patients with inconclusive AET values.5 However, their usefulness depends on the type of symptoms reported. In our study, approximately 73% of the patients with typical symptoms (with or without concomitant atypical symptoms) had a positive reflux–symptom association, while more than 63% of the patients with isolated atypical symptoms had a negative reflux–symptom association. Among the patients with laryngopharyngeal symptoms, a positive reflux–symptom association was found in fewer than 10% of the cases. The utility of SI and SAP may be limited due to the challenges in determining the onset of certain symptoms, such as hoarseness.5,19 Additionally, 4.4% of all patients did not mark any symptoms during the pH‑impedance monitoring. Therefore, in some cases, relying solely on the reflux–symptom association analysis could be misleading,5,20 and the assessment of MNBI and / or number of reflux episodes may be more useful for a definitive GERD diagnosis. MNBI, a marker of mucosal integrity, plays a role in differentiating GERD phenotypes. Abnormal values have been shown to predict the response of extraesophageal symptoms to PPI therapy.21-24 In our study, MNBI correlated negatively with both AET and the number of reflux episodes. Two‑thirds of the patients with isolated atypical symptoms had normal MNBI, as compared with only one‑third of those with isolated typical symptoms. In the patients with isolated atypical symptoms and inconclusive AET values, the diagnosis of GERD was primarily based on the presence of abnormal MNBI and / or number of reflux episodes. Since baseline impedance can be lower in nonreflux inflammation or motility disorders (eg, eosinophilic esophagitis, achalasia), this adjunctive parameter may be useful when EGD and manometry performed prior to reflux monitoring have excluded such abnormalities (as in our study).
Careful evaluation of the causes of extraesophageal symptoms is advised, as such symptoms may be due to GERD or alternative disorders. Even in patients diagnosed with GERD, it can be difficult to establish whether reflux is the principal cause of the symptoms.4,25 Of note, we analyzed the presence of conclusive GERD in patients with atypical symptoms only after prior evaluation by other specialists, including laryngologists. We did not focus on laryngoscopic signs of reflux, as GERD should not be diagnosed based on laryngoscopy alone.4,25 Calabrese et al18 reported pathological laryngoscopy findings in 71% of the patients with extraesophageal symptoms, but the GERD prevalence was similar in their cohort, regardless of whether laryngoscopy findings were positive or negative.
A significant overlap between GERD and functional disorders complicates patient management.9,26-30 Among individuals with GERD, around 31% met the criteria for at least 2 other functional condidtions, mostly functional dyspepsia and irritabile bowel syndrome.9,26 One‑third of our patients reported abdominal pain with poor association with reflux, regardless of AET values. Although reflux monitoring is not typically recommended for epigastric / abdominal pain, these symptoms may be mischaracterized or overlap with heartburn.5 Indeed, reflux monitoring is useful when functional heartburn, reflux hypersensitivity, supragastric belching, or rumination is suspected.5,30 In our study, functional heartburn accounted for approximately 42% of the heartburn cases, and was found to be 4 times more common in the patients with normal AET, as compared with those with abnormal AET values. Approximately 23% of the individuals with regurgitation and normal AET had a negative reflux–symptom association. Moreover, belching was the most commonly reported atypical symptom, and showed a negative association with reflux in about half of the patients. These findings highlight the high prevalence of a functional background of troublesome symptoms, a distinction that is clinically relevant, as it shifts the treatment away from PPIs and antireflux surgery toward behavioral therapy and neuromodulators.
The role of EGD in GERD diagnosis was limited in this study, as the inclusion of EGD findings in addition to reflux monitoring increased the number of patients with conclusive GERD by only 2.7%. A total of 84% of the patients had no objective endoscopic evidence of GERD. The low prevalence of esophagitis could be related to prior PPI therapy, as the data regarding PPI use or withdrawal at the time of EGD were not documented. Many individuals use PPI before undergoing EGD, which further limits its reliability in identifying objective GERD.
Nevertheless, our results are particularly relevant for re‑evaluating the clinical importance of symptom assessment as the primary indicator of GERD presence and the basis for PPI initiation. Conclusive GERD findings were present in only 29% of all patients with troublesome symptoms referred for reflux monitoring. Specifically, GERD was diagnosed in approximately half of the patients reporting isolated typical symptoms, one‑third of those with both typical and atypical symptoms, and fewer than one‑fifth of the individuals with isolated atypical symptoms. The low prevalence of confirmed GERD in a large cohort of patients with isolated atypical symptoms, even after the exclusion of other causes, strongly supports current recommendations against routine PPI prescription, even though their use remains common in clinical practice. Furthermore, the high prevalence of functional heartburn among the patients with typical symptoms highlights the need for confirming GERD objectively through reflux monitoring before initiating maintenance therapy.
- Vakil N, van Zanten SV, Kahrilas P, et al; Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence‑based consensus. Am J Gastroenterol. 2006; 101: 1900‑1920. | Crossref
- Savarino E, de Bortoli N, De Cassan C, et al. The natural history of gastro‑esophageal reflux disease: a comprehensive review. Dis Esophagus. 2017; 30: 1‑9. | Crossref
- El‑Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro‑oesophageal reflux disease: a systematic review. Gut. 2014; 63: 871‑880. | Crossref
- Katz PO, Dunbar KB, Schnoll‑Sussman FH, et al. ACG Clinical Guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2022; 117: 27‑56. | Crossref
- Gyawali CP, Yadlapati R, Fass R, et al. Updates to the modern diagnosis of GERD: Lyon Consensus 2.0. Gut. 2024; 73: 361‑371. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION