The 2025 updated European Resuscitation Council guidelines: overview of the most important changes
Key words: cardiac arrest, guidelines, resuscitation, systems saving lives



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The 2025 updated European Resuscitation Council guidelines: overview of the most important changes
The new resuscitation guidelines of the European Resuscitation Council were published in October 2025. The aim of the guidelines is to sustainably improve the survival rate after cardiac arrest through structured and evidence‑based care systems. The latest update brings about some important changes and innovations. In this review, we highlighted the new recommendations, especially in the chapters on adult advanced life support, post‑resuscitation care, and the role of systems in saving lives. The importance of the first 3–5 minutes after cardiac arrest has been further strengthened. The most relevant updates include, among others, the need for lay people to be educated in cardiopulmonary resuscitation (CPR) by physicians, the role of the dispatch center in helping the caller identify cardiac arrest and ventilation failure, identification of the intravenous access as superior to other routes of drug administration, highlighting the possibility of vector change in defibrillation, importance of provider experience in the context of point‑of‑care ultrasound use, and the role of sedation during CPR.
Introduction
The latest version of the European Resuscitation Council (ERC; www.erc.edu) resuscitation guidelines was published in October 2025. The guidelines are updated every 5 years based on the International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science of the International Liaison Committee on Resuscitation. The current version of the ERC guidelines is divided into the following sections: Epidemiology, Systems Saving Lives, Adult Basic Life Support (BLS), Adult Advanced Life Support (ALS), Pediatric Life Support (PLS), Neonatal Life Support (NLS), Special Circumstances in Resuscitation, Post‑Resuscitation Care, Education for Resuscitation, Ethics in Resuscitation, and First Aid.1 The guidelines are based on available worldwide scientific evidence. The latest document includes several content updates and extensions: new recommendations in the chapter Systems Saving Lives, highlighting the importance of the first 3–5 minutes following cardiac arrest, updates in the chapter on ALS regarding defibrillation strategies and airway management, and new recommendations in the chapter on post‑resuscitation care concerning, among other aspects, temperature control and determining the cause of cardiac arrest. The target audience of the ERC guidelines includes bystanders, emergency medical service providers, hospital staff, teachers, instructors, health organizations, policymakers, and anyone interested in improving survival after cardiac arrest. The European bystander cardiopulmonary resuscitation (CPR) rate is 58%, with regional variations ranging from 13% to 82%.1
Systems Saving Lives: new recommendations
The chapter Systems Saving Lives has gained particular importance in the new guidelines. Introduced in 2021, it discusses topics such as telephone‑assisted CPR, bystander CPR campaigns, school‑based CPR education (the Kids Save Lives initiative), first‑responder systems, and cardiac arrest centers (CACs). The strong evidence supporting these interventions, particularly focusing on the most critical first 3–5 minutes following cardiac arrest, has been further reinforced. In the 2025 guidelines, the updated Chain of Survival includes prevention, early recognition of cardiac arrest, and activation of emergency response in the first ring. The second ring comprises early bystander CPR and defibrillation. The third ring represents ALS and post‑resuscitation care, whereas the fourth ring includes recovery of quality of life and rehabilitation after cardiac arrest (Figure 1).2,3
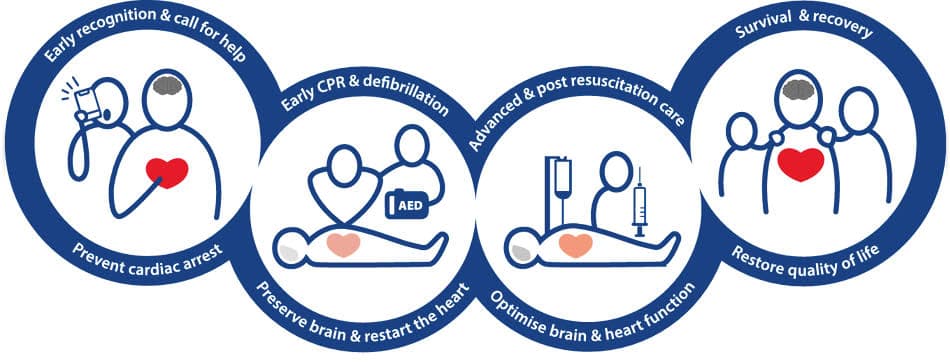
Abbreviations: AED, automated external defibrillator; CPR, cardiopulmonary resuscitation
The topics of social media, advocacy, health policy activities, and the use of artificial intelligence (AI) are addressed for the first time in the new guidelines. Active use of social media is recommended to increase public awareness of resuscitation and support training initiatives. Digital technologies and AI are identified as promising future tools to improve early recognition of cardiac arrest and post‑resuscitation care, although further research is needed to confirm their practical benefit. Advocacy efforts aim to encourage policymakers and authorities to implement strategies that improve cardiac arrest survival, such as national and international awareness campaigns for lay people, mandatory CPR education in schools, and sustainable bystander training initiatives, with the focus on the key first 3–5 minutes after the collapse.2
Furthermore, specialized treatment of nontraumatic out‑of‑hospital cardiac arrest (OHCA) patients in CACs is recommended, along with the establishment of regional networks and protocols to ensure coordinated care. In addition, it is suggested that health care systems establish local protocols for developing and maintaining a network for cardiac arrest management. This time, not only are transport recommendations made, but also greater emphasis is placed on establishing more targeted regional care structures and enhancing networking between them, with the aim of improving treatment outcomes in the long term.2 For example, in Germany, this is already guaranteed nationwide by certification of specialized hospitals as CACs (Figure 2).4
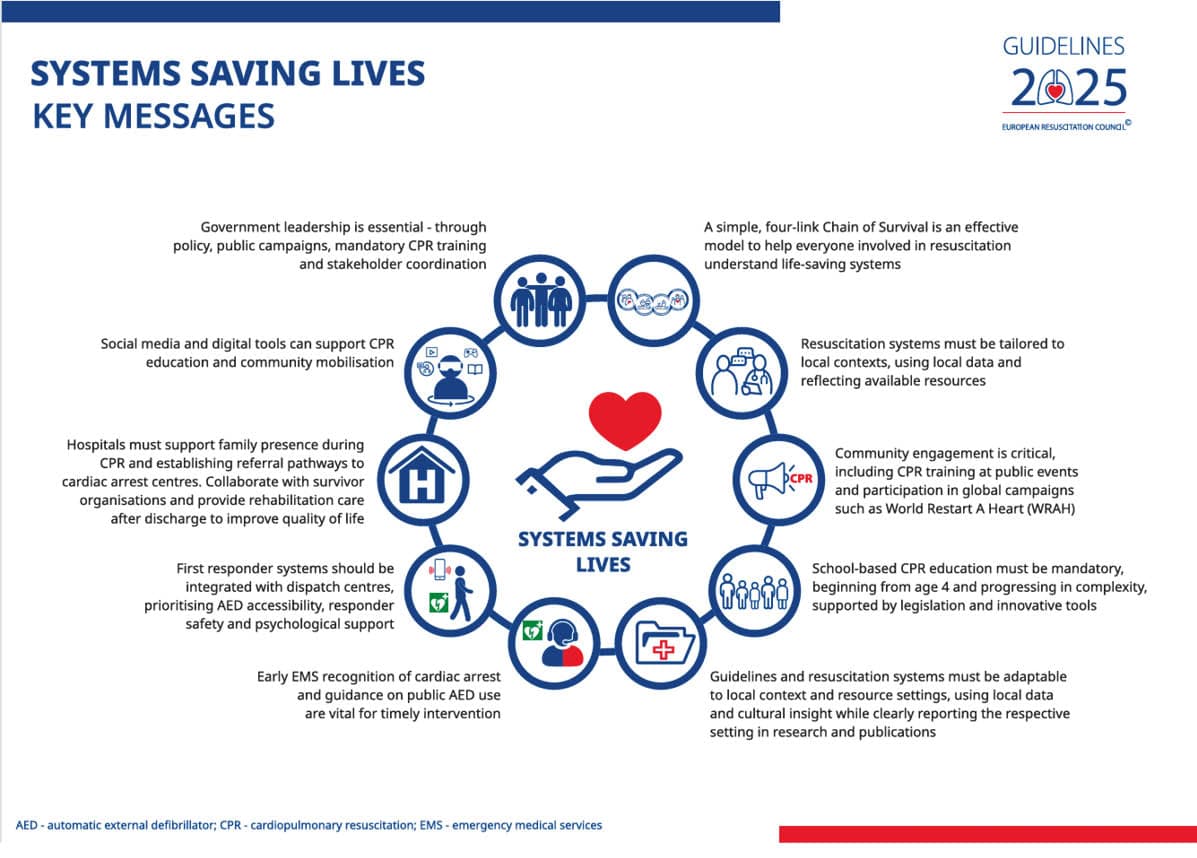
Abbreviations: EMS, emergency medical services; others, see Figure 1
Changes in other chapters
The chapters on BLS, education, and ethics do not introduce novel recommendations, but they do place new emphasis on certain aspects. In the chapter on BLS, the role of emergency dispatchers is strongly emphasized, particularly in early recognition of abnormal breathing and cardiac arrest—this should be performed by lay people during or after calling for help and together with the dispatcher—and immediate initiation of telephone‑assisted CPR using standardized criteria.5 The Education for Resuscitation chapter focuses on training methods tailored to different target groups, such as children of different ages, and highlights the importance of diverse educational approaches, including blended learning, self‑directed learning, and serious games for teaching resuscitation skills.6 The chapter on ethics highlights the importance of protecting the mental health of first responders, including the routine provision of appropriate support structures.7 The PLS and NLS chapters include a new dedicated section on pediatric cardiac arrest in special situations, and more clearly delineate resuscitation approaches. The section on PLS also includes a novel Check–Call–CPR suggestion, now more aligned with the suggestions concerning adults.8,9 The chapter on cardiac arrest in special circumstances now offers more detailed and adapted algorithms (thrombolysis during CPR in suspected or proven pulmonary embolism, lipid resuscitation in local anesthetic intoxication, no resuscitative endovascular balloon occlusion of the aorta in traumatic cardiac arrest, etc.) and illustrations, along with changes in BLS and ALS protocols to further optimize resuscitation in specific situations.10
Updates to the chapter on advanced life support
For all clinicians participating in or leading cardiac arrest procedures, the chapter concerning ALS in adults is of key relevance. The updated guidelines introduce a new section on ALS in settings with limited resources. Even in highly developed health care systems, resuscitation may also take place under constrained conditions, such as remote environments, adverse weather, or mass‑casualty incidents. In these situations, prevention of cardiac arrest and prioritization of first aid and BLS are emphasized. Limited availability of personnel and equipment may adversely affect outcomes following cardiac arrest during ALS.11
Consciousness during resuscitation is a newly addressed issue—in selected cases, emergency medical services may consider light analgesia and sedation to reduce awareness, pain, and distress in patients who regain consciousness during CPR. Increased cerebral perfusion and oxygenation, particularly during high‑quality CPR, may contribute to conscious or subconscious perception. Medication use in such cases should follow local protocols (Figure 3).11
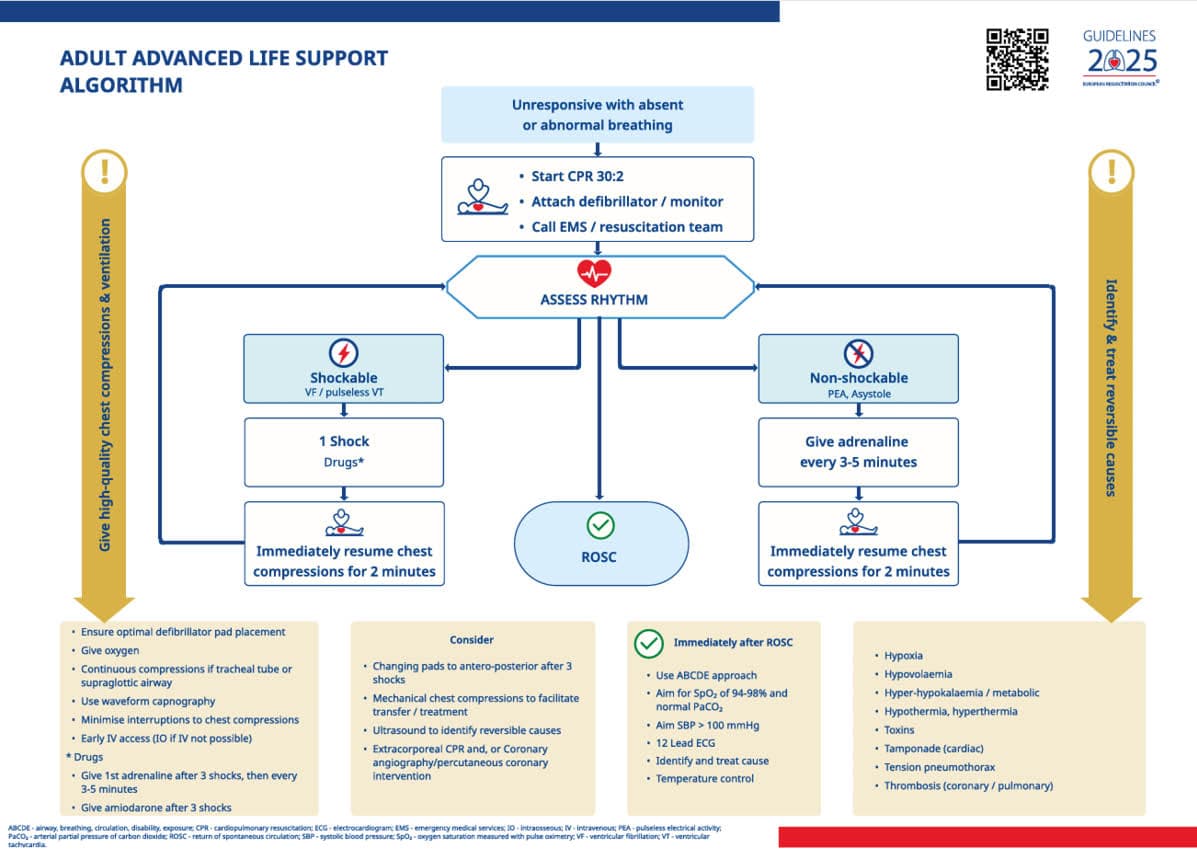
Abbreviations: ABCDE, airway, breathing, circulation, disability, exposure; ECG, electrocardiogram; IO, intraosseous; IV, intravenous; PaCO2, arterial partial pressure of carbon dioxide; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation; SBP, systolic blood pressure; SpO2, oxygen saturation measured with pulse oximetry; VF, ventricular fibrillation; VT, ventricular tachycardia; others, see Figures 1 and 2
Defibrillation strategies and airway management
When appropriate expertise is available, manual defibrillation is preferred over automated external defibrillator use due to faster rhythm analysis and treatment. ALS providers must be proficient in both modalities. Defibrillation is recommended even in very fine ventricular fibrillation, as it may result in return of spontaneous circulation (ROSC).11 Advances in extracorporeal CPR include smaller and more mobile veno‑arterial extracorporeal membrane oxygenation (VA‑ECMO) systems, allowing their earlier use in specialized centers and, in selected cases, prehospital settings. Extracorporeal CPR may be considered for selected patients when conventional resuscitation is unsuccessful.11 The importance of regular electrocardiography (ECG) training is emphasized to minimize rhythm misinterpretation and treatment errors. Recommendation regarding initial electrode placement remains unchanged; the electrodes should be placed antero‑lateral, with careful positioning of 1 electrode at the cardiac apex. In refractory shockable rhythms, an anteroposterior defibrillation vector may be considered after 3 unsuccessful shocks.
Effective bag‑mask ventilation is still considered sufficient, with a 2‑person technique preferred. Supraglottic airway placement or endotracheal intubation should not cause significant interruptions to chest compressions and should be performed only by experienced providers. Mechanical ventilation must always be confirmed as effective; otherwise, effective manual ventilation should be resumed. Ventilation efficacy should always be verified by reliable indicators, such as visible chest rise, as inadequate ventilation remains common (particularly during bag‑mask ventilation) and affects survival.11
Physiologically‑guided resuscitation
The 2025 guidelines highlight that a sudden decrease in end‑tidal CO2 (ETCO2) may indicate recurrent cardiac arrest or severely reduced cardiac output. Chest compressions should be resumed in adults if systolic blood pressure falls below 50 mm Hg despite interventions. In patients with continuous invasive arterial blood pressure monitoring, small intravenous adrenaline doses (eg, 50–100 µg) are recommended instead of a 1‑mg bolus. If no response occurs after a cumulative dose of 1 mg, extravasation should be excluded before administering additional 1‑mg doses every 3–5 minutes. Target values during resuscitation are equal to or greater than 30 mm Hg for diastolic arterial pressure and equal to or greater than 25 mm Hg (3.3 kPa) for ETCO2.11
Point‑of‑care ultrasound may be used during ongoing resuscitation by experienced providers to identify potentially reversible causes and to optimize the chest compression technique. Its use must not in any way compromise compression quality or cause delays. Intravenous access is the preferred route for drug administration during cardiac arrest in adults. If intravenous access cannot be rapidly established, intraosseous access is recommended. Routine administration of calcium (strong recommendation against for OHCA and weak recommendation against for in‑hospital cardiac arrest), sodium bicarbonate (weak recommendation against), or corticosteroids during resuscitation is not advised unless there are specific indications for their use.11 Health care systems should establish structured pathways for the aftercare of cardiac arrest survivors and their relatives, covering the continuum from hospital discharge to follow‑up. The care should be multidisciplinary and aligned with the needs of the patients and their families, with appropriate training and ongoing education opportunities for health care professionals. The updated in‑hospital algorithm now clearly differentiates between patients with and without existing circulation.11
Overall, the guidelines emphasize prioritization of high‑quality chest compressions with effective ventilation, early defibrillation, rapid identification and treatment of reversible causes, and administration of adrenaline in nonshockable cardiac arrest.
Updates in post‑resuscitation care
The chapter on post‑resuscitation care was developed jointly by the European Society of Intensive Care Medicine and the ERC, in close collaboration. In particular, it includes changes in temperature management, neurological outcome prognostication, and rehabilitation / aftercare, as well as clarification of the possible genetic causes of unexplained cardiac arrests. The recommendations on rehabilitation and follow‑up care after discharge from hospital have been supplemented. For neurological prognosis, the prognostic algorithm is expanded, and specific indicators of neurological outcomes are presented.12 Recent guideline updates introduce substantial modifications to post‑resuscitation management, which are of particular relevance to cardiology practice. The focus is on post‑resuscitation care pathways and system‑level approaches to improve survival (Figure 4).12
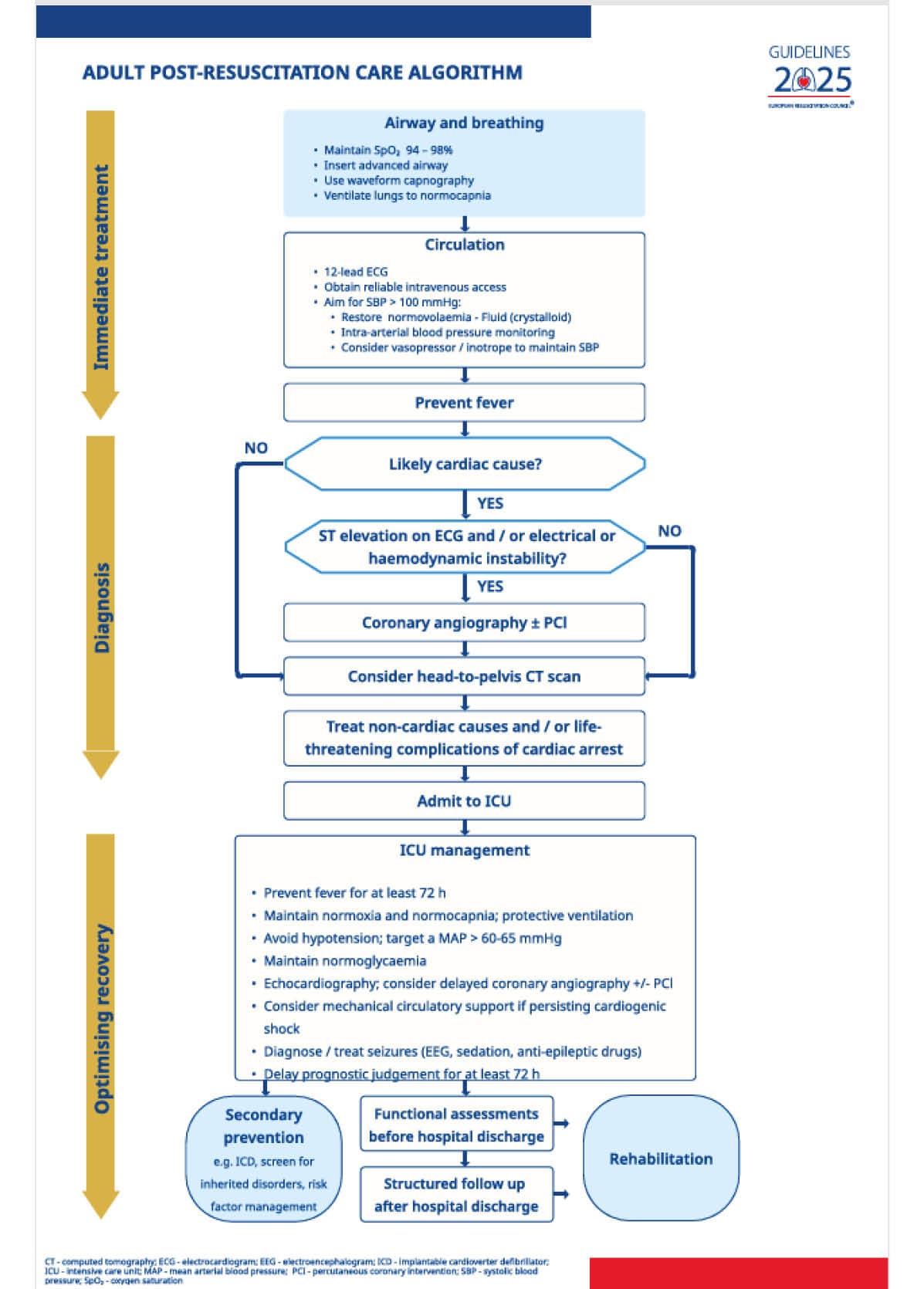
Abbreviations: CT, computed tomography; EEG, electroencephalogram; ICD, implantable cardioverter‑defibrillator; ICU, intensive care unit; MAP, mean arterial blood pressure; PCI, percutaneous coronary intervention; others, see Figure 3
Determining the cause of cardiac arrest
Early clarification of the underlying etiology is highlighted as a key preventive strategy. In patients with suspected acute coronary syndromes, coronary angiography remains the preferred initial investigation, particularly in the presence of ST‑segment elevation. In patients without ST‑segment elevation, priority is given to comprehensive biphasic whole‑body computed tomography (CT) imaging, including CT pulmonary angiography (eg, to identify hemorrhage or pulmonary embolus). If coronary angiography fails to identify a causative lesion, further neurothoracic imaging is recommended. In the cases of unexplained cardiac arrest, the diagnostic workup has been substantially expanded. The recommended investigations now include toxicological and genetic testing (Brugada syndrome, long QT syndrome), serial 12‑lead ECG, cardiac magnetic resonance imaging (as needed), sodium channel blocker testing (to detect Brugada syndrome), exercise testing, and analysis of data from implantable or wearable monitoring devices. Identification of inherited conditions requires extension of diagnostic evaluation to family members to reduce the risk of OHCA in relatives.12 Resuscitation‑related injuries should be actively sought (including on CT). Following ROSC, oxygen therapy should initially be delivered at a high concentration and then carefully titrated to avoid both hypo- and hyperoxia. Target oxygen saturation level remains at 94%–98%, corresponding to a partial pressure of arterial oxygen value of 75–100 mm Hg. The updated guidelines explicitly address reduced accuracy of pulse oximetry in individuals with darker skin pigmentation (overestimation). Ventilation strategies continue to aim for normocapnia.12 Special attention is required in hypothermic patients, in whom hypocapnia may occur more easily. Blood gas analysis should therefore be interpreted accordingly, using either temperature‑corrected or uncorrected values. Most intensive care recommendations from earlier versions of the guidelines remain valid. Comatose patients should undergo airway protection with endotracheal intubation performed by experienced clinicians. Initial mechanical ventilation may begin with 100% oxygen, followed by rapid adjustment once reliable oxygenation measurements are available. Hypoxia must be strictly avoided. Postarrest hemodynamic management prioritizes the prevention of hypotension, with a target mean arterial pressure value above 60–65 mm Hg. Volume therapy, vasopressors, and inotropes should be selected according to individual hemodynamic requirements. Routine corticosteroid administration is discouraged. In selected patients with favorable prognostic indicators and persistent cardiogenic shock or recurrent malignant ventricular arrhythmias, escalation to mechanical circulatory support may be appropriate if pharmacological therapy proves insufficient. Available options include intra‑aortic balloon counterpulsation, ventricular assist devices, and VA‑ECMO.12 Management of periarrest arrhythmias has been revised. Prophylactic antiarrhythmic medication is no longer recommended in the patients who remain free of arrhythmias after ROSC. Standard intensive care measures continue to apply, including cautious use of antibiotics, preference for short‑acting sedatives, avoidance of routine neuromuscular blockade, head‑of‑bed elevation, stress ulcer prophylaxis, maintenance of normoglycemia, seizure management, and deferral of neurological prognostication for at least 72 hours.12
Temperature control and neurological recovery
The concept of temperature control has replaced earlier terminology related to targeted temperature management. In comatose patients, active prevention of fever is recommended, with body temperature maintained at or below 37.5 °C for 36–72 hours after ROSC. Patients who present with mild spontaneous hypothermia (32–36 °C) should not be actively rewarmed. Prehospital cooling using large volumes of cold intravenous fluids is no longer advised. The benefit of inducing moderate hypothermia (32–34 °C) in specific patient groups remains uncertain, as such groups have not yet been clearly identified. While ERC recommendations are cautious in this regard, recent Cochrane data suggest a significant neurological benefit without increased adverse events with therapeutic hypothermia at 32–34 °C for at least 24 hours, and the topic remains controversial.12 Continuous electroencephalography (EEG) monitoring remains central for the detection of subclinical seizures. Antiepileptic therapy should be initiated only in the presence of clinical or electrographic seizure activity, with levetiracetam or sodium valproate recommended alongside sedation. The guidelines newly emphasize that awakening attempts may be appropriate in patients with posthypoxic myoclonus and a benign EEG pattern several days after cardiac arrest. Multimodal prognostication remains the cornerstone of outcome assessment. While individual tests may be initiated earlier, final prognostic conclusions should not be drawn earlier than 72 hours after cardiac arrest, and only in the absence of confounding factors.12 A poor neurological outcome is considered likely only when multiple unfavorable predictors are present, including absent brainstem reflexes, bilaterally absent N20 responses, highly malignant EEG patterns, sustainably elevated and / or increasing neuron‑specific enolase levels, persistent status myoclonus, or extensive anoxic brain injury on neuroimaging. Decisions regarding withdrawal of life‑sustaining treatment must be clearly separated from neurological outcome prediction. Such decisions should integrate neurological findings with patient age, comorbidities, overall organ function, and documented patient preferences. Transparent communication within the care team and with relatives is essential.12
Rehabilitation, follow‑up, and long‑term outcomes
Postdischarge care has been strengthened through expanded recommendations on rehabilitation and structured follow‑up. Early rehabilitation measures initiated in the intensive care unit (ICU), including mobilization, delirium prevention strategies, and ICU diaries, are encouraged. Optimally, prior to discharge, patients should undergo a comprehensive evaluation of physical, cognitive, and psychological sequelae to guide personalized rehabilitation planning. Assessment of neurological recovery is no longer limited to conventional outcome scales but should include more detailed functional evaluations before discharge and during the first 3 months thereafter. Relatives are to be actively involved throughout both diagnostic clarification and the rehabilitation process.12 The guidelines recommend systematic consideration of organ donation in all patients approaching end of life. In comatose, ventilated patients after cardiac arrest, the possibility of organ donation should be integrated into end‑of‑life decision‑making. All organ donations following resuscitation should be documented in national resuscitation registries. For example, in Germany, organ donation after cardiac arrest requires formal confirmation of brain death, making early initiation of brain death diagnostics essential. Other countries apply different legal standards for donation after circulatory death.12
Conclusions
The 2025 ERC guidelines emphasize the interaction of multiple systems and stakeholders. The Systems Saving Lives chapter and the updated Chain of Survival underscore the importance of prevention (mostly in the in‑hospital setting), early intervention, and specialized follow‑up care to improve survival after cardiac arrest, highlighting the crucial importance of the interventions within the first 3–5 minutes after OHCA.
The most relevant changes include the following: 1) the first 3–5 minutes following cardiac arrest are of key importance; 2) physicians need to educate lay people in CPR; 3) the dispatch center is required to help the person calling for help identify cardiac arrest and ventilation failure; 4) successful ventilation by professionals needs to be ensured; 5) intravenous access is superior to other access methods, and vector change in defibrillation is possible; 6) point‑of‑care ultrasound is to be used only by experienced providers; 7) sedation during CPR should be considered; 8) temperature management is still controversial; 9) use of multimodal neuroprognostication is encouraged; 10) rehabilitation and / or organ donation strategies should be applied; 11) genetic testing in younger cardiac arrest victims should be facilitated; and 12) the Check–Call–CPR recommendation now also applies to children.
- Greif R, Lauridsen KG, Djärv T, et al. European Resuscitation Council Guidelines 2025: executive summary. Resuscitation. 2025; 215: 110770. | Crossref
- Semeraro F, Schnaubelt S, Olasveengen TM, et al. European Resuscitation Council Guidelines 2025: systems saving lives. Resuscitation. 2025; 215: 110821. | Crossref
- Bricoli S, Aschieri D, Niccoli G. How to better prevent sudden cardiac death? Recent advances. Pol Arch Intern Med. 2024; 134: 16838. | Crossref
- Rott N, Reinsch L, Böttiger BW. Cardiac arrest centers improve survival. Curr Opin Crit Care. 2025; 31: 713‑716. | Crossref
- Smyth MA, van Goor S, Hansen CM, et al. European Resuscitation Council Guidelines 2025: adult basic life support. Resuscitation. 2025; 215: 110771. | Crossref
ARTICLE INFORMATION