Three-dimensional catheter ablation of atypical atrial flutter in a lung transplant recipient

 CC BY 4.0
CC BY 4.0
Three-dimensional catheter ablation of atypical atrial flutter in a lung transplant recipient
We present a case of a patient with a history of dual lung transplant (LTx) and heart failure exacerbation due atypical left‑sided atrial flutter (AFl), successfully treated with 3‑dimensional (3D) catheter ablation (CA).
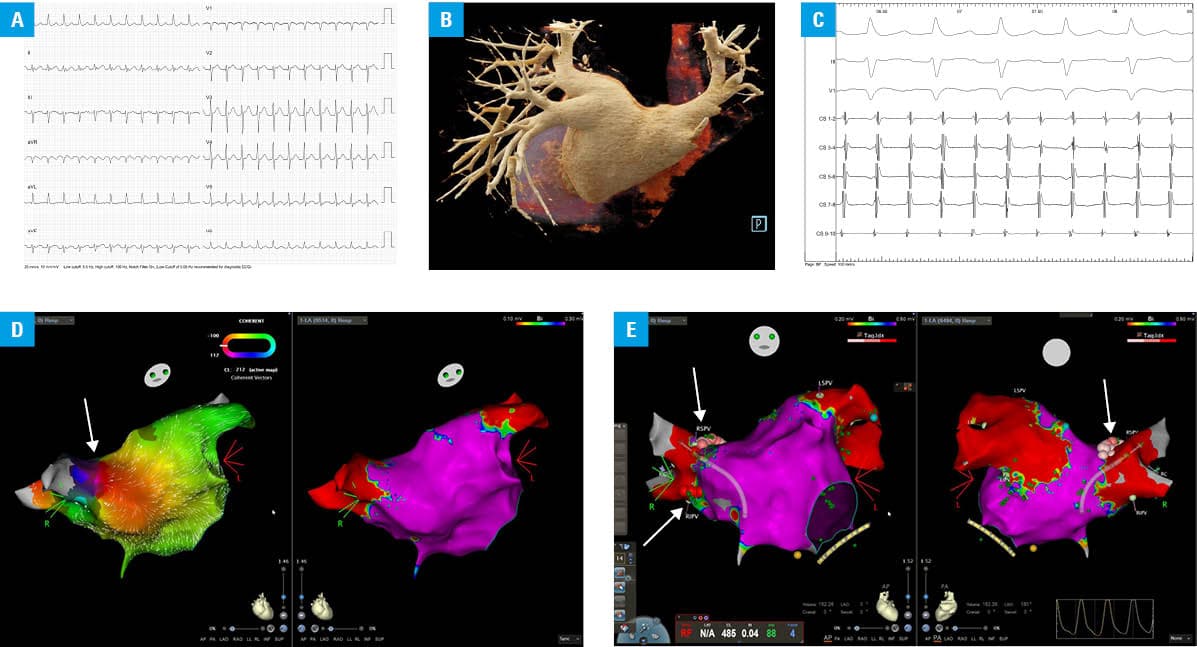
A 62‑year‑old man, after dual LTx (April 2023) due to hypersensitivity pneumonitis, with a history of hypertension and iatrogenic adrenal insufficiency, was hospitalized due to shortness of breath at rest. On Holter electrocardiography, we observed supraventricular tachycardia with an average heart rate of 129 bpm (min, 118 bpm; max, 134 bpm), which turned out to be AFl on 12‑lead electrocardiography (Figure 1A). On echocardiography, mild left ventricular (LV) hypertrophy and no impairment of LV systolic function were identified (LV ejection fraction, 65%; LV internal diameter at end‑diastole, 47 mm; interventricular septum diastolic thickness, 12 mm). Due to N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) level increased to a maximum value of 9018 pg/ml (reference range <125 pg/ml), heart failure exacerbation was diagnosed. The patient was qualified for 3D CA (CARTO, Biosense Webster, Diamond Bar, California, United States). Because of the history of LTx, cardiac computed tomography angiography with reconstruction of the left atrium (LA) was performed perioperatively (Figure 1B). Based on activation (a classical Figure‑of‑eight macro‑reentry circuit) and voltage mapping, atypical AFl related to the anastomosis of the right‑sided pulmonary veins and LA was identified and successfully ablated (Figure 1C–1E). The ablation lesion set was navigated with the use of an activation and voltage maps. Each application was delivered with a power of 40 W, guided by the Ablation Index algorithm (Figure 1E; red dots, 550; pink dots, 380). Exit block was confirmed by pacing around the right‑sided pulmonary veins, and noninducibility of arrhythmia was tested with repetitive aggressive burst pacing from the coronary sinus catheter at the end of the procedure. No isoproterenol or atropine challenges were performed. During 3‑month follow‑up, no recurrence of AFl was observed on Holter electrocardiography, no heart palpitations were reported by the patient, his exercise tolerance improved, and NT‑proBNP values dropped to a minimum of 740 pg/ml. Unfortunately, 5 months after the procedure, the patient was hospitalized due to pneumonia, atrial fibrillation and multiple organ failure, which ultimately led to his death.
Atrial arrhythmias (AAs) remain an independent mortality risk factor, especially in patients with most advanced comorbidities.1 AA after LTx is one of the biggest challenges in this novel treatment of advanced lung diseases, and occurs in up to 20%–35% of the recipients.2 The most common early AA after LTx is atrial fibrillation; however, over time, the prevalence of atrial tachycardia and AFls drastically increases. The incidence rate of these late AAs after dual LTx is 4.1% per year.3 Even though dual LTx should provide isolation of the pulmonary veins from the LA, electrical connections between the graft and the recipient myocardial tissue are observed.4 These connections can be a potential cause of AA and should be a target for ablation. Preoperative imaging and 3D mapping are crucial for the safety and effectiveness of this procedure. Long‑term outcomes seem to be promising, with a cumulative arrhythmia‑free survival rate of 75% at a median follow‑up of 19 months.5 To our knowledge, this is the first case of atypical AFl after LTx treated with 3D CA in Poland.
- Mitrega K, Sredniawa B, Sokal A, et al. Does the atrial fibrillation still increase the risk of death? Results from the NOMED study in one‑year follow‑up. Pol Arch Intern Med. 2024; 134: 16619. | Crossref
- Marazzato J, Eikermann M, Di Biase L. Management of atrial arrhythmias after lung transplant. JACC Clin Electrophysiol. 2023; 9: 1824‑1835. | Crossref
- Saglietto A, Matta M, Gaita F, et al. Late atrial arrhythmias after lung transplantation: a meta‑analysis. J Cardiovasc Med (Hagerstown). 2020; 21: 577‑582. | Crossref
- Baykaner T, Cooper JM. Atypical flutter following lung transplantation involving recipient‑to‑donor tissue connections. HeartRhythm Case Rep. 2018; 4: 548‑552. | Crossref
- Mariani MV, Pothineni NVK, Arkles J, et al. Catheter ablation of atrial arrhythmias following lung transplant: electrophysiological findings and outcomes. J Cardiovasc Electrophysiol. 2021; 32: 49‑57. | Crossref
ARTICLE INFORMATION