Association between serum amino acid profiles and clinical severity in heart failure with reduced ejection fraction: an exploratory study

 CC BY 4.0
CC BY 4.0
Association between serum amino acid profiles and clinical severity in heart failure with reduced ejection fraction: an exploratory study
Introduction
Heart failure (HF) is one of the leading epidemiologic challenges worldwide.1-3 Its pathophysiology, which involves activation of the inflammatory system, has been widely investigated in recent studies.4,5 In contrast, the metabolic background of HF has not yet been thoroughly examined.
Amino acids play key roles in whole‑body energy homeostasis, muscle metabolism, and mitochondrial function at the cellular level, and these processes may be particularly relevant in HF with reduced ejection fraction (HFrEF). Numerous biomarkers have been proposed for diagnosing HF and predicting disease progression. Still, their clinical utility remains largely observational. Although these markers are supported by strong rationale, they have not yet been integrated into effective therapeutic modulation.
The aim of the present study was to investigate the association between serum amino acid profiles and clinical severity in patients with HFrEF. Our objective was to provide a systemic and metabolic perspective on HFrEF, and to address the existing data gap regarding the link between comprehensive amino acid profiling and disease severity.
Patients and methods
This observational, prospective study was conducted in patients with stable HFrEF as an exploratory, hypothesis‑generating analysis. Laboratory testing, including amino acid profiling, was performed on admission, after 12 hours of fasting. All patients subsequently underwent echocardiographic examination and coronary angiography. Serum concentrations of 33 amino acids were quantified using liquid chromatography–tandem mass spectrometry with the MassChrom Amino Acid Analysis kit (Chromsystems, Gräfelfing, Germany; Supplementary material, Methodology). Individuals with food allergies, restrictive diets, or kidney dysfunction were excluded from the analysis.
The study was approved by the Institutional Ethics Committee of the Poznan University of Medical Sciences (113/21). Written informed consent was obtained from all participants.
Statistical analysis
Normality of variable distribution was assessed using the Shapiro–Wilk test. Variables not following a normal distribution are described as median with interquartile range (IQR), while categorical variables are presented as number and percentage. Group comparisons were performed using the Mann–Whitney test or Kruskal–Wallis test, as appropriate. Categorical variables were compared using the χ2 test or Fisher exact test when applicable.
Associations between amino acid concentrations and clinical variables were evaluated using the Spearman rank correlation coefficient (R). As a broad panel of amino acids was analyzed, adjustment for multiple comparisons was performed using the Benjamini–Hochberg false discovery rate (FDR) procedure. Both unadjusted P values and FDR‑adjusted Q values were evaluated. Statistical significance was defined as a P value below 0.05, with Q values below 0.05 considered significant after FDR correction.
To address potential confounding, a simple multivariable logistic regression model was built for New York Heart Association (NYHA) functional class equal to or greater than II. The model included leucine concentration as the main predictor, and was adjusted for age, sex, and creatinine level as clinically relevant covariates. A receiver operating characteristic (ROC) analysis was performed. Given the limited sample size, no additional variables were included to avoid overfitting.
Statistical analyses were performed using JASP software (version 0.14.1, University of Amsterdam, Amsterdam, the Netherlands).
Results
A total of 50 consecutive patients (31 men) at a median (IQR) age of 67 (62–72) years were admitted for planned hospitalization due to HF symptoms following referral by a cardiologist.
The clinical status was assessed according to the NYHA functional classification, and was distributed as follows: class I/II, 16 patients (32%), class II, 24 patients (48%), class II/III, 3 patients (6%), and class III, 7 patients (14%).
Baseline demographic and clinical characteristics of the participants, along with laboratory test results and pharmacotherapy on admission, are presented in Supplementary material, Table S1. Concentrations of all 33 analyzed amino acids across the study groups are shown in Supplementary material, Table S2. The results of correlation analyses assessing the relationship between NYHA functional class and selected amino acids, before and after FDR correction, are presented in Supplementary material, Table S3.
Spearman correlation analysis identified several associations between amino acid concentrations and clinical parameters. After adjustment for multiple comparisons using the Benjamini–Hochberg FDR procedure, only leucine remained significantly associated with NYHA functional class (R = –0.6; P <0.001; Q = 0.03; Figure 1A).
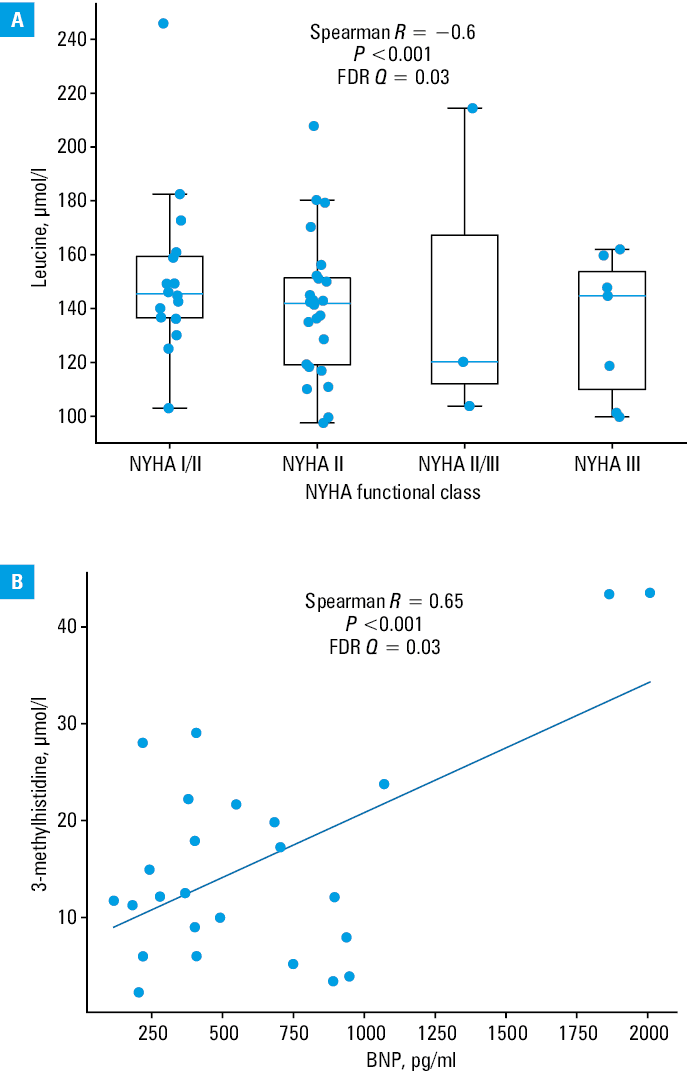
A positive correlation between circulating 3‑methylhistidine concentration and B‑type natriuretic peptide (BNP) levels after adjustment for multiple comparisons was noted (R = 0.65; P <0.001; Q = 0.03; Figure 1B and Supplementary material, Table S3).
In the multivariable analysis adjusted for age, sex, and creatinine level, leucine remained independently associated with NYHA functional class equal to or greater than II (odds ratio, 0.93 per 1-µmol/l increase; 95% CI, 0.89–0.97; P = 0.002), indicating that higher leucine levels were linked with lower odds of impaired functional status. ROC curve analysis for leucine as a predictor of NYHA class equal to or greater than II yielded an area under the curve of 0.85, with sensitivity of 60% and specificity of 92%. The covariates were selected a priori based on clinical relevance to minimize confounding, and the direction of the association in the multivariable model was consistent with the inverse correlation observed in the univariable analysis.
Discussion
Our prospective, exploratory study investigated the relationship between serum amino acid profiles and clinical severity in patients with HFrEF. We observed a relationship between a circulating amino acid (leucine) and markers of disease severity, including NYHA functional class and BNP levels. The inverse association between leucine and NYHA functional class suggests that leucine may reflect metabolic reserve or anabolic capacity rather than the disease burden itself.
Our findings suggest a potential link between HF and catabolic status associated with metabolic stress.6,7 The observed effects were mild to modest, but consistent with the severity of clinical symptoms. This hypothesis‑generating study demonstrates an association between clinical status, left ventricular systolic function, established HF biomarkers (eg, BNP), and serum amino acid profiles. After correction for multiple comparisons using the FDR method, the association between NYHA functional class and leucine level remained significant, while the remaining correlations should be interpreted with caution.
The observed association between lower circulating leucine levels and worse NYHA functional class could not be explained by age, sex, or renal function. This finding supports the independent relationship between leucine concentration and functional status. According to our results, for each 1-µmol/l increase in the leucine concentration, the odds of having a NYHA class equal to or greater than II decreased by 7%.
These associations reflect metabolic disturbances characterized by increased catabolism and dysregulation of branched‑chain amino acid (BCAA) metabolism, potentially contributing to an elevated cardiometabolic risk and worsening clinical status.8
The inverse relationship between the level of leucine, a BCAA, and clinical severity in HFrEF may reflect alterations in metabolic pathways associated with systemic catabolic state in HF and increased oxidative stress.9 These findings may result from disturbances in BCAA metabolism that were previously reported in HF.10,11
In our study, lower leucine concentrations were associated with worse functional status, suggesting increased metabolic demand or altered amino acid utilization in patients with more advanced disease. In an animal model, a relationship between leucine consumption, macrophage activation, and elevated cardiovascular risk was reported.12 Our findings suggest an association between circulating leucine levels and functional assessment (NYHA classification), circulating 3‑methylhistidine levels, and biochemical markers (such as BNP).
Overall, the results of this exploratory analysis support the biological plausibility that altered BCAA metabolism is associated with disease severity in HFrEF. Given the cross‑sectional design, these findings should be interpreted as associative and do not imply causality.
Importantly, our analysis supports the concept of HFrEF as a systemic disease, characterized by enhanced catabolic activity extending beyond the myocardium. This hypothesis parallels the concept of myocardial “metabolic remodeling,” while emphasizing whole‑body metabolic involvement.13
We also observed a positive association between 3‑methylhistidine and BNP levels. Unlike leucine, 3‑methylhistidine is not incorporated into newly synthesized proteins but is instead released during the degradation of actin and myosin in skeletal muscle.14 Elevated serum concentrations of 3‑methylhistidine in patients with HFrEF may reflect increased myofibrillar protein breakdown and may serve as a marker of worse functional status, frailty, and muscle wasting.15
These findings underscore the value of comprehensive metabolic profiling over reliance on individual biomarkers, and suggest potential clinical implications for the monitoring and risk stratification in HFrEF. In our hypothesis‑generating analysis, 2 circulating amino acids were identified as significant for predicting the clinical status of HFrEF patients. After correction for multiple comparisons, only leucine remained significantly associated with NYHA functional class and only 3‑methylhistidine remained associated with BNP levels.
Limitations
This prospective study included a limited number of patients and employed a cross‑sectional design. The absence of a control group represents an important limitation. Given the exploratory nature of the study and the relatively small sample size, the statistical power was limited. Although correction for multiple comparisons using the FDR method was applied, the results should be interpreted as hypothesis‑generating and require confirmation in larger cohorts. Potential confounders, such as diabetes mellitus, kidney function parameters, or applied pharmacotherapy, may have influenced circulating amino acid concentrations. Other residual confounding cannot be excluded despite adjustment for selected covariates.
The novelty of this study lies in the comprehensive profiling of serum amino acids as metabolic markers of HFrEF severity.
Conclusions
In this exploratory study, lower circulating leucine levels were independently associated with worse functional status in patients with HFrEF. These findings suggest that alterations in amino acid metabolism may reflect systemic metabolic impairment in HF. However, given the cross‑sectional design, these results should be considered exploratory, and require confirmation in larger studies.
- Khan MS, Shahid I, Bennis A, et al. Global epidemiology of heart failure. Nat Rev Cardiol. 2024; 21: 717‑734. | Crossref
- Galas A, Morawiec R, Tymińska A, et al. Implementation of recommendations regarding pharmacotherapy optimization in patients with heart failure with reduced ejection fraction undergoing scheduled hospitalization: the HEROES study. Pol Arch Intern Med. 2025; 135: 17135. | Crossref
- Rywik TM, Wiśniewska A, Cegłowska U, et al. Heart failure with reduced, mildly reduced, and preserved ejection fraction: outcomes and predictors of prognosis. Pol Arch Intern Med. 2023; 133: 16522. | Crossref
- Han H, Xu J, Zhou Z, et al. Inflammatory mechanisms and targeted drugs in heart failure. Clin Exp Hypertens. 2026; 48: 2608225. | Crossref
- Yu Z, Wang J, Zheng F, et al. Prediabetes‑related inflammatory biomarkers modulate left ventricular diastolic function in patients with heart failure with preserved ejection fraction. Pol Arch Intern Med. 2025; 135: 17021. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION