Use of a bioresorbable scaffold in a patient with chronic limb-threatening ischemia: the first successful implantation in Poland

 CC BY 4.0
CC BY 4.0
Use of a bioresorbable scaffold in a patient with chronic limb-threatening ischemia: the first successful implantation in Poland
A 69‑year‑old man with a history of hypertension, type 2 diabetes mellitus complicated by neuropathy, and significant tobacco use (over 40 pack‑years) presented to a vascular medicine outpatient clinic with suspected ischemic diabetic right foot syndrome. Physical examination showed necrosis involving the entire second toe and part of the first toe. Doppler ultrasound demonstrated absent blood flow in the anterior tibial artery (ATA) and posterior tibial artery (PTA), confirmed by a low ankle‑brachial index of 0.23 and toe‑brachial index of 0.03, with a toe pressure of 5 mm Hg. A diagnosis of chronic limb‑threatening ischemia was established, and the patient was referred for urgent revascularization.
Initial angiography identified no significant lesions in the femoral or popliteal regions. A high origin of the PTA was observed, which was patent proximally the rest of the artery was completely occluded. An atypical tibioperoneal trunk connecting the ATA and fibular artery was patent and exhibited no narrowing. The ATA was occluded throughout its course except at the ostium. The fibular artery was patent and free of stenosis. In its distal segment, it divided into multiple branches supplying the lateral and medial plantar arteries as well as smaller vessels (Figure 1A and 1B).
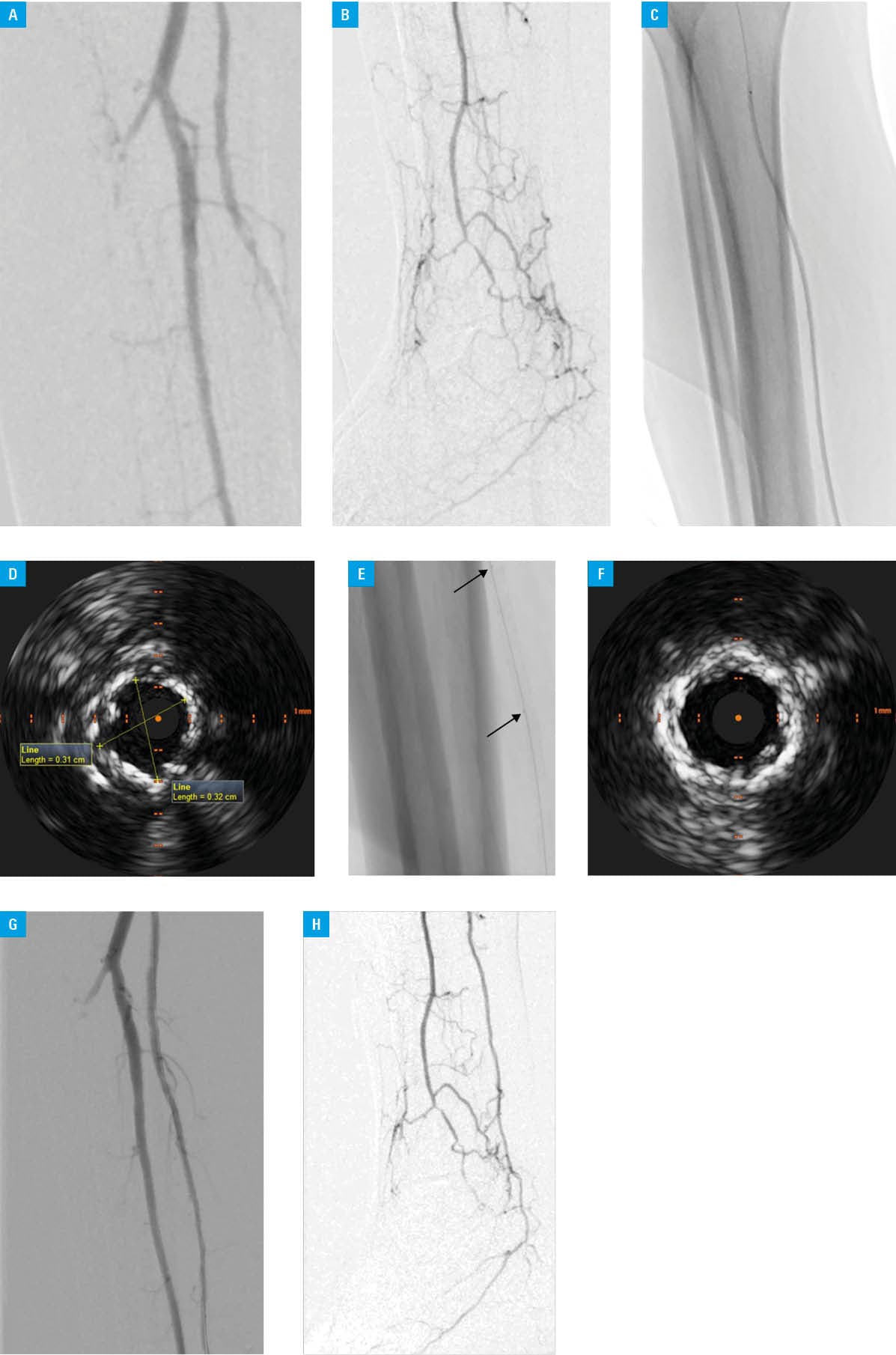
A V‑18 Control guidewire (Boston Scientific, Marlborough, Massachusetts, United States) and a 2.5‑mm Passeo‑18 balloon catheter (Biotronik AG, Baar, Switzerland) were used to recanalize the PTA, and angioplasty was performed successfully (Figure 1C). Intravascular ultrasound (IVUS) demonstrated significant dissection in the PTA wall, with a vessel diameter of up to 3.2 mm (Figure 1D). Vessel preparation for stenting was conducted with a noncompliant 3 mm × 40 mm RX Solarice balloon catheter (Medtronic, Minneapolis, Minnesota, United States). The Esprit BTK bioresorbable drug‑eluting (everolimus) scaffold (Abbott, Abbott Park, Illinois, United States), 3 mm × 38 mm, was selected due to the elevated risk of long‑term complications associated with conventional stent use in this lesion area. The scaffold was successfully deployed and gradually expanded (2 atm every 5 s) to the target diameter of 3.2 mm, with target pressure maintained for 30 seconds (Figure 1E). The noncompliant balloon was used again to ensure optimal stent apposition. IVUS confirmed proper placement and expansion of the Esprit scaffold (Figure 1F). Final angiography demonstrated restored blood flow through the PTA and improved contrast filling of the plantar arteries, resulting in enhanced perfusion of the forefoot region (Figure 1G and 1H).
At 1‑month follow‑up, after the second right toe amputation, the patient demonstrated significant healing progress. Doppler US confirmed adequate blood flow through the PTA, with no stenosis in the treated area. Complete wound healing was observed at 3‑month follow‑up.
This clinical case describes the first implantation of a bioresorbable scaffold in peripheral arteries in Poland. The procedure was completed successfully, and the outcome was assessed on IVUS due to the radiolucency of the implanted scaffold, which is not visible on standard fluoroscopy.1 Clinical success was achieved, as restoration of blood flow facilitated healing of the ischemic wound and prevented major limb amputation. These findings suggest that this technology may reduce the rate of reocclusion in below‑the‑knee arteries, which can occur due to rupture and deformation of conventional drug‑eluting stents.2
- Secemsky EA, Armstrong EJ, Chandra V, et al. Contemporary chronic limb‑threatening ischemia care in the United States—part 2: designing clinical device trials. J Soc Cardiovasc Angiogr Interv. 2025; 4: 103934. | Crossref
- DeRubertis BG, Varcoe RL, Krishnan P, et al. Drug‑eluting resorbable scaffold versus balloon angioplasty for below‑the‑knee peripheral artery disease: 2‑year results from the LIFE‑BTK Trial. Circulation. 2025; 152: 1076‑1086. | Crossref
ARTICLE INFORMATION