Cervical Nabothian cyst mimicking metastatic disease on post-therapy iodine-131 single-photon emission computed tomography / computed tomography



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Cervical Nabothian cyst mimicking metastatic disease on post-therapy iodine-131 single-photon emission computed tomography / computed tomography
Thyroid cancer is the most common endocrine malignancy.1 Distant metastases from differentiated thyroid cancer are uncommon, and usually involve the lungs or bones. Therefore, unexpected iodine‑131 (131I) uptake at atypical sites should prompt careful evaluation to exclude false‑positive findings.2
A 40‑year‑old woman with papillary thyroid carcinoma, stage pT1aNx, underwent total thyroidectomy in September 2024. In June 2025, she was admitted for radioiodine treatment under recombinant human thyroid‑stimulating hormone (rhTSH) stimulation. Before rhTSH administration, her TSH level was 0.01 mIU/l (reference range [RR], 0.35–4.94 mIU/l), serum thyroglobulin level was 1.42 ng/ml (RR, 3.68–64.15 ng/ml), and antithyroglobulin antibody level was 1.2 IU/ml (RR, <4.11 IU/ml). Forty‑eight hours after rhTSH stimulation, the level of TSH exceeded 100 mIU/l and the level of stimulated thyroglobulin was 53.48 ng/ml. At 96 hours, the values decreased to 37.17 mIU/l and 48.61 ng/ml, respectively. The patient received 100 mCi (3.7 GBq) of 131I.
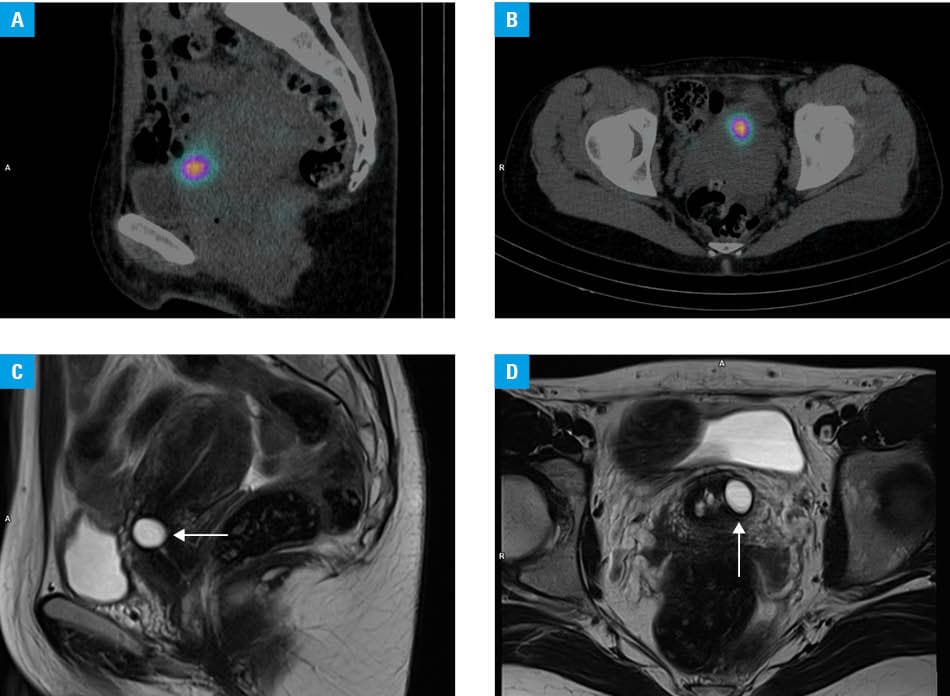
Post‑therapy whole‑body imaging demonstrated bilaterally increased 131I uptake in the thyroid bed (remnant thyroid tissue), as well as additional superior midline activity, probably corresponding to the pyramidal lobe remnant. Additional pelvic single‑photon emission computed tomography / computed tomography (SPECT/CT) identified 2 foci of increased uptake: a 14‑mm hypodense focus in the uterine body, left of the midline, and a slightly hypodense area up to 19 mm on the right of the uterine cervix. No suspicious lymph node activity or other extrapelvic abnormal foci were reported. On fused images, the dominant area of increased tracer uptake was localized to the uterine cervix (Figure 1A and 1B). Given the atypical site for differentiated thyroid cancer spread and the existence of rare reports of true cervical involvement, urgent gynecologic evaluation was performed.3 Transvaginal ultrasonography showed a benign Nabothian cysts. Pelvic magnetic resonance imaging (MRI) confirmed a sharply marginated, T2‑hyperintense cervical cyst at the site of the cervical radioiodine uptake, consistent with the Nabothian cyst (Figure 1C and 1D).
Cervical radioiodine uptake is a recognized pitfall on postradioiodine imaging of differentiated thyroid cancer. In a cohort undergoing neck‑to‑pelvis SPECT/CT, uterine cervical uptake was observed in 26.3% of women (n = 76), and in all patients who underwent pelvic MRI, the uptake was localized to a Nabothian cysts.4 In another case series focusing on abnormal activity detected proximally from the urinary bladder, most patients presented with uptake localized to the cervix on SPECT/CT, which corresponded to Nabothian cysts on transvaginal ultrasonography.5 The exact mechanism remains unclear; however, given the characteristics of these cysts, a plausible explanation is retention of radioiodine‑containing mucus or secretions within the cystic space.
Awareness of this entity and diagnostic confirmation with pelvic hybrid imaging and targeted gynecologic workup may prevent misclassification as metastatic disease and unnecessary escalation of therapy.
- Ringel MD, Sosa JA, Baloch Z, et al. 2025 American Thyroid Association management guidelines for adult patients with differentiated thyroid cancer. Thyroid. 2025; 35: 841‑985. | Crossref
- Song H‑J, Xue Y‑L, Qiu Z‑L, Luo Q‑Y. Uncommon metastases from differentiated thyroid carcinoma. Hell J Nucl Med. 2012; 15: 233‑240. | Crossref
- Kim MJ, Jung H, Park CS. Papillary thyroid cancer with suspicious uterine cervix metastasis: a case report and literature review. Gland Surg. 2022; 11: 1270‑1278. | Crossref
- Isoda T, BaBa S, Maruoka Y, et al. Nabothian cyst a predominant cause of false‑positive iodine uptake in uterus: comparison of SPECT/CT and pelvic MRI. Clin Nucl Med. 2014; 39: 680‑684. | Crossref
- Liu S, Zhang M, Pan Y, et al. Nabothian cyst associated with high false‑positive incidence of iodine‑131 uptake in whole‑body scans after treatment for differentiated thyroid cancer. Nucl Med Commun. 2013; 34: 1204‑1207. | Crossref
ARTICLE INFORMATION