Increasing use of cardiac implantable electronic devices (CIEDs) has led to a parallel rise in the number of patients requiring end‑of‑service CIED management.1-4 As global populations age, growing numbers of patients reach elderliness and form a group in which decision‑making is often multifactorial and complex. Although the definition of elderliness is heterogenous and not limited to chronological age, patients aged 80 years or older generally meet this criterion. Nevertheless, despite the recommendations to not routinely consider advanced age as one of the most important risk factors for periprocedural complications of transvenous lead extraction (TLE), clinical concerns persist regarding whether advanced age itself should be considered a limiting factor when referring patients for this procedure.1,5,6
In this issue of Polish Archives of Internal Medicine, Drożdż et al7 present a comprehensive meta‑analysis evaluating the safety and efficacy of TLE in patients aged 80 years or older vs those younger than 80 years. Data from 17 studies including nearly 16 000 patients, of whom 17.6% were 80 years or older, were pooled, demonstrating procedural success rates exceeding 96% in both age groups, without significant differences in major or minor procedural complications. In‑hospital mortality was comparable in octogenarians and younger patients. Although these findings add to the evidence suggesting that advanced age alone should not be considered a contraindication for TLE, several questions remain open.
First, in daily practice, TLE is usually performed in the context of complex scenarios, most commonly cardiac device–related infectious endocarditis (CDRIE), lead or system malfunction, or vascular complications, for example, venous thrombosis.3,4 In elderly patients, these situations frequently occur in the presence of substantial comorbidity, including active cancer and frailty. Clinical decision‑making is therefore often guided by experience rather than evidence, as frail and very elderly patients remain underrepresented in major clinical trials and registries that form the basis of evidence‑based medicine, and when patients aged 80 years or older are included, they likely represent a highly selected subgroup.4,8,9
Among the iddues that need to be considered, 2 key questions guide the clinical decision: whether the patient truly requires TLE and whether the indication for device therapy is still valid, as shown in Figure 1.
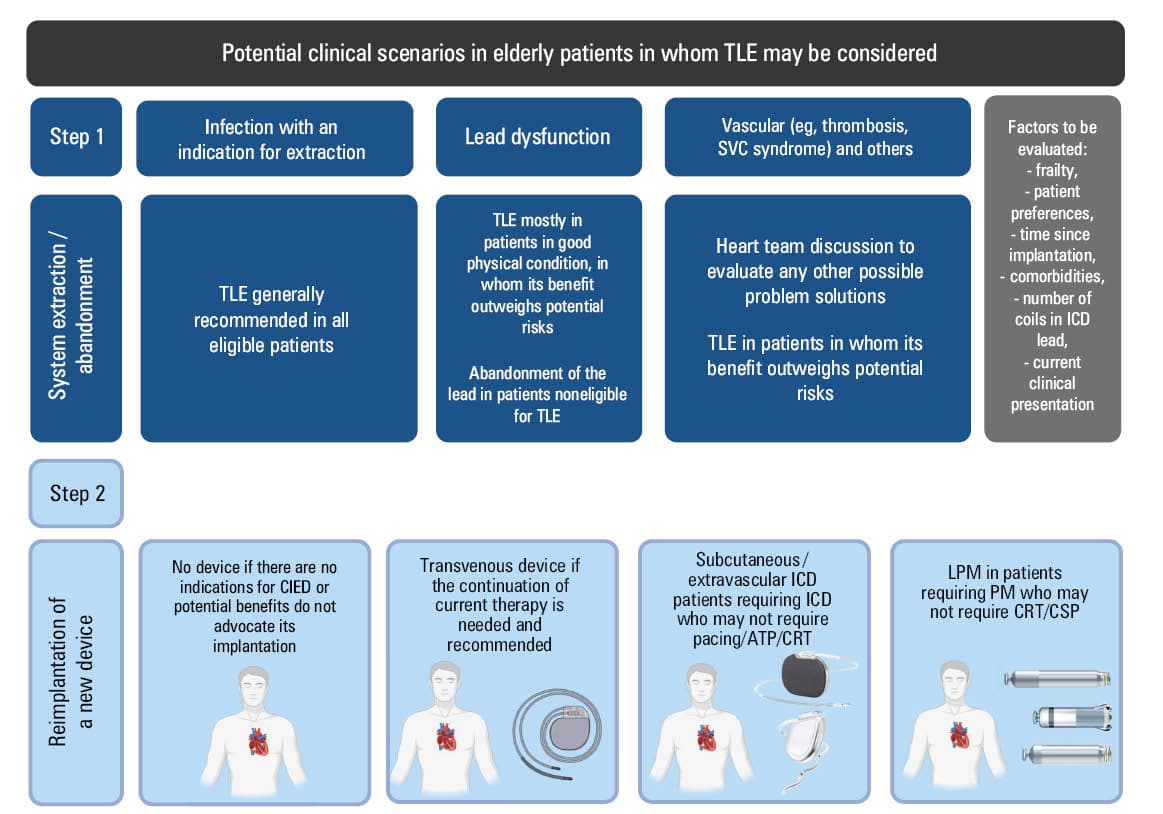
Abbreviations: ATP, antitachycardia pacing; CIED, cardiac implantable electronic device; CRT, cardiac resynchronization therapy; CSP, conduction system pacing; ICD, implantable cardioverter‑defibrillator; LPM, leadless pacemaker; SVC, superior vena cava; TLE, transvenous lead extraction
Regarding indications for TLE, in patients with CDRIE, mortality risk is high; thus, once the systemic device‑related infection is confirmed, TLE should be performed whenever feasible. The procedure should be undertaken as early as clinically possible, while considering the patient clinical condition, time since implantation, and other factors associated with worse periprocedural outcomes, such as lead age, number of implantable cardioverter‑defibrillator (ICD) coils, degree of adhesion calcification, or renal failure.3,10,11 In selected cases, such as large vegetations or failed TLE, surgical extraction may be required and should be considered by a heart team, particularly when performed electively.
When TLE is considered for noninfectious indications, the decision is often less straightforward. For example, extraction of an isolated dysfunctional defibrillation lead may increase procedural complexity if other leads are damaged periprocedurally, whereas implantation of a new lead with abandonment of the malfunctioning one may appear a simpler and safer alternative. Although not evaluated in this meta‑analysis, such a strategy may be particularly attractive in elderly, multimorbid, or frail patients due to perceived procedural risks, and is often used in settings with limited access to TLE, although long‑term outcome data remain scarce. However, abandoned leads may compromise future venous access, increase infection risk, and complicate subsequent diagnostic evaluation (eg, magnetic resonance imaging conditionality) and management. Conversely, TLE may restore venous patency and enable future device therapy but introduces a procedural risk that must be considered in the context of the overall clinical condition. Vascular indications, such as venous thrombosis, superior vena cava syndrome, or the need for device upgrade in the absence of patent venous access may strongly favor TLE after careful patient evaluation. Importantly, chronological age alone, as suggested by Drożdż et al,7 provides limited guidance in this complex decision‑making process. Frailty, functional status, or patient cognitive function further influence the expected benefit of continued device therapy, yet these variables are rarely incorporated into formal risk stratification models used to guide decisions regarding complex procedures.
Once the decision to extract the leads has been made, the optimal reimplantation strategy must be determined. Although in the majority of patients, the continuation of previously implanted type of device may be chosen, a non‑negligible percentage of patients may no longer require device therapy. Those may include, for instance, patients with improvement of left ventricular ejection fraction who previously had an ICD as a form of primary prevention of sudden cardiac death, or those with reversible causes of conduction disturbances who no longer require permanent pacing. For patients undergoing TLE because of device‑related infection, the risk of recurrent CDRIE is higher. In that context, the nontransvenous systems have substantially expanded possible therapeutic options. Leadless pacemakers may offer an attractive solution in selected patients requiring ventricular, and recently, dual‑chamber pacing.12,13 The nontransvenous ICDs, either subcutaneous ICD (sICD) or extravascular ICD, may provide defibrillation therapy without intracardiac hardware. In certain clinical scenarios, combining these technologies, although challenging, may allow for avoiding reimplantation of transvenous leads.14,15 However, these strategies are not without limitations, and, for example, the size of the sICD generator may discourage its implantation in elderly frail patients, making such a decision particularly challenging.
The authors of the discussed meta‑analysis7 appropriately acknowledged limitations of their methodology, yet several uncertainties remain regarding the optimal strategy for elderly patients considered for TLE, including anticipated survival, quality of life, and patient preferences. The development of practical tools integrating frailty assessment, comorbidity burden, and functional status may help optimize this process. In many cases, shared decision‑making with patients and their families becomes key to align therapeutic strategies with patient expectations.
The key message of this analysis is clear: advanced age alone should not be considered a contraindication to TLE. When performed in experienced centers, TLE can be carried out safely and effectively even in, most likely carefully selected, very elderly patients. As the populations age and the use of CIED therapy increases, the number of octogenarians requiring TLE will inevitably rise. The future challenges will not simply be to demonstrate procedural safety, but to develop refined risk stratification strategies that integrate frailty, comorbidity burden, and patient‑centered outcomes.
- Tajstra M, Dyrbuś M, Kowalski O, et al. Transvenous leadless pacemaker extraction: when, who, where, and how? Pol Heart J. 2026; 84: 174‑187. | Crossref
- Jacheć W, Polewczyk A, Nowosielecka D, Kutarski A. Clinical profile and outcomes among patients with cardiac implantable electronic device presenting as isolated pocket infection, pocket‑related infective endocarditis, or lead‑related infective endocarditis. Europace. 2025; 27: euaf053. | Crossref
- Blomström‑Lundqvist C, Traykov V, Erba PA, et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections‑endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS). Europace. 2020; 22: 515‑549. | Crossref
- Bongiorni MG, Burri H, Deharo JC, et al. 2018 EHRA expert consensus statement on lead extraction: recommendations on definitions, endpoints, research trial design, and data collection requirements for clinical scientific studies and registries: endorsed by APHRS/HRS/LAHRS. Europace. 2018; 20: 1217. | Crossref
- Keene D, Nielsen JC, Burri H, et al. Cardiac implantable electronic device upgrades and downgrades: a Clinical Consensus Statement of the European Heart Rhythm Association (EHRA) of the ESC, the Asia Pacific Heart Rhythm Association (APHRS), Canadian Heart Rhythm Society (CHRS), Heart Rhythm Society (HRS), and the Latin American Heart Rhythm Society (LAHRS). Europace. 2025; 27: euaf252. | Crossref
ARTICLE INFORMATION