
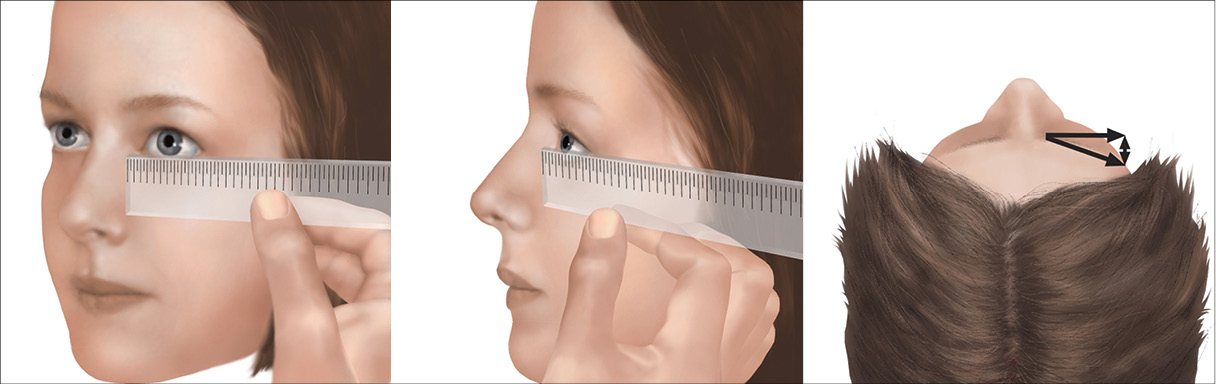
Ryc. 5. Technika pomiaru szerokości szpary powiekowej za pomocą linijki (autorka ryciny: Magdalena Wolnicka-Maryniak)
Należy zachować ostrożność przy diagnozowaniu dzieci <6. tygodnia życia, szczególnie noworodków, ze względu na fizjologiczne odrębności w tym okresie (np. obrzęk powiek).
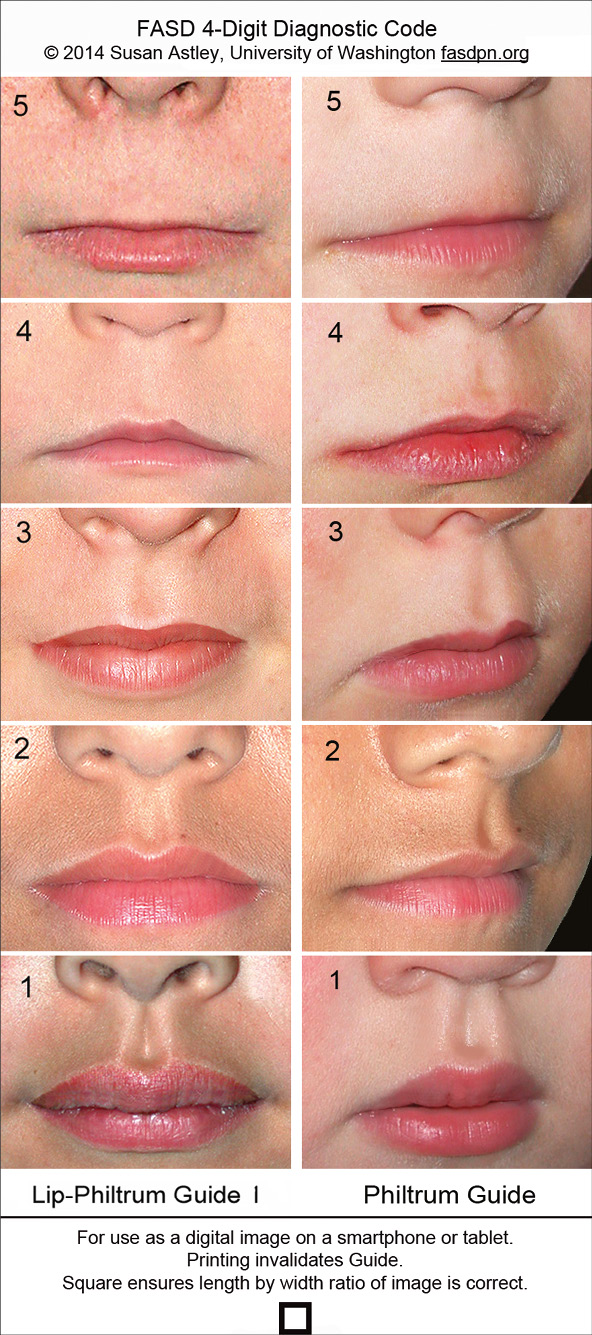
Ryc. 6. Skala obrazkowa LPG (lip‑philtrum guide) © 2020 Susan (Astley) Hemingway PhD, University of Washington
Rynienka podnosowa i warga górna
Inaczej niż w przypadku szerokości szpary powiekowej, ocena rynienki podnosowej i wargi górnej (dokładnie czerwieni wargowej) jest w poszczególnych ośrodkach klinicznych i badawczych ujednolicona. Ocenę przeprowadza lekarz za pomocą 5-stopniowej obrazkowej skali LPG (lip-philtrum guide [ryc. 6]).28 Rynienkę podnosową oraz wargę górną dziecka należy porównać ze zdjęciami przedstawionymi na skali. W trakcie oceny dziecko powinno zachować neutralny wyraz twarzy, natomiast twarz badającego musi się znajdować na wysokości twarzy pacjenta (ryc. 7). Za nieprawidłowe uznaje się wartości 4 i 5 dla obu parametrów.
W przypadku pacjentów czarnoskórych należy wykorzystywać skalę obrazkową odpowiednią dla tej grupy.29
U pacjentów pochodzenia azjatyckiego oraz z innych grup etnicznych decyzję o wyborze narzędzia podejmuje lekarz wykonujący badanie. W dokumentacji medycznej należy odnotować informację o braku swoistych narzędzi diagnostycznych.
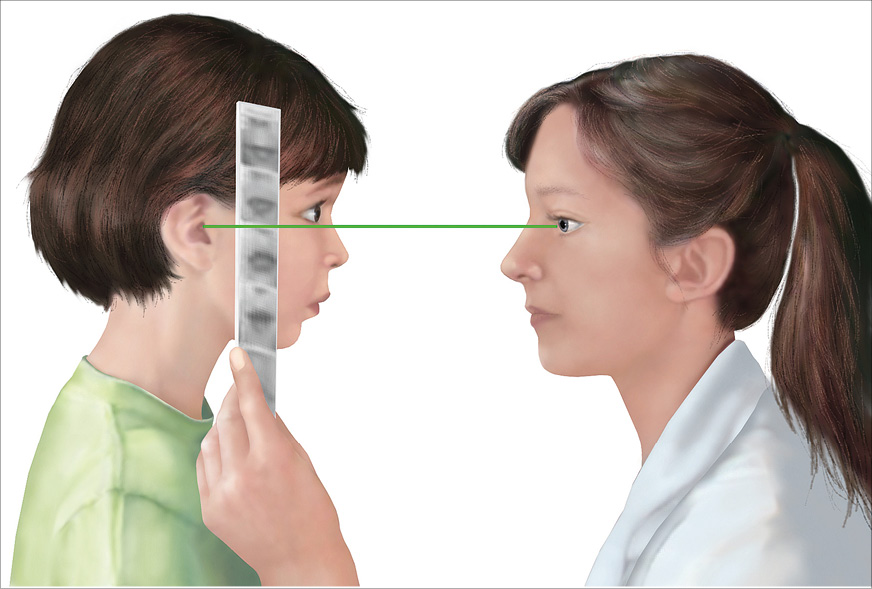
Ryc. 7. Pozycja umożliwiająca właściwą ocenę wargi górnej i rynienki podnosowej za pomocą skali LPG
(autorka ryciny: Magdalena Wolnicka‑Maryniak)
Diagnostyka różnicowa
W przypadku niejednoznacznego obrazu klinicznego (np. współistnienia dysmorfii nietypowych dla FASD), wad rozwojowych narządów wewnętrznych, znacznego opóźnienia rozwoju psychoruchowego i intelektualnego lub dodatniego wywiadu rodzinnego w kierunku chorób genetycznych pacjenta należy skierować na konsultację do genetyka klinicznego, który podejmie decyzję o przeprowadzeniu diagnostyki genetycznej.30 Diagnostyka różnicowa FASD obejmuje zespoły genetyczne oraz inne embriopatie31 (p. załącznik 6).
Piśmiennictwo:
1. Reid N., Hayes N., Young S.B. i wsp.: Caregiver-reported physical health status of children and young people with fetal alcohol spectrum disorder. J. Dev. Orig. Health Dis., 2021; 12 (3): 420–4272. Ayoub L., Aring E., Gyllencreutz E. i wsp.: Visual and ocular findings in children with fetal alcohol spectrum disorders (FASD): validating the FASD Eye Code in a clinical setting. BMJ Open Ophthalmol., 2023; 8 (1): e001215
3. Ludwików K., Westerlund A., Al-Taai N. i wsp.: Dentofacial characteristics of children and adolescents with foetal alcohol spectrum disorders: a comparison with matched controls. Prog. Orthod., 2023; 24 (1): 46
4. Himmelreich M., Lutke C.J., Hargrove E.T.: The lay of the land: Fetal Alcohol Spectrum Disorder (FASD) as a whole-body diagnosis. W: In The Routledge Handbook of Social Work and Addictive Behaviors. Taylor & Francis Group, 2020
5. Kable J.A., Mehta P.K., Coles C.D.: Alterations in insulin levels in adults with prenatal alcohol exposure. Alcohol Clin. Exp. Res., 2021; 45 (3): 500
6. Kable J.A., Mehta P.K., Rashid F. i wsp.: Path analysis of the impact of prenatal alcohol on adult vascular function. Alcohol Clin. Exp. Res., 2022; 47 (1): 116
7. Dyląg K.A., Anunziata F., Bandoli G. i wsp.: Birth defects associated with prenatal alcohol exposure: a review. Children (Basel), 2023; 10 (5): 811
8. Ustawa z dnia 5 grudnia 1996 r. o zawodach lekarza i lekarza dentysty, art. 2 ust. 1 (t.j. Dz.U. z 2019 poz. 537 ze zm.)
9. Del Campo M., Jones K.L.: A review of the physical features of the fetal alcohol spectrum disorders. Eur. J. Med. Genet., 2017; 60 (1): 55–64
10. Carey J.C., Cohen M.M., Curry C.J.R. i wsp.: Elements of morphology: standard terminology for the lips, mouth, and oral region. Am. J. Med. Genet. A, 2009; 149A (1): 77–92
11. Allanson J.E., Cunniff C., Hoyme H.E. i wsp.: Elements of morphology: standard terminology for the head and face. Am. J. Med. Genet. A, 2009; 149A (1): 6–28
12. Allanson J.E., Biesecker L.G., Carey J.C. i wsp.: Elements of morphology: introduction. Am. J. Med. Genet. A, 2009; 149A (1): 2–5
13. Biesecker L.G., Aase J.M., Clericuzio C. i wsp.: Elements of morphology: standard terminology for the hands and feet. Am. J. Med. Genet. A, 2009; 149A (1): 93–127
14. Hunter A., Frias J.L., Gillessen-Kaesbach G. i wsp.: Elements of morphology: standard terminology for the ear. Am. J. Med. Genet. A, 2009; 149A (1): 40–60
15. Hennekam R.C.M., Cormier-Daire V., Hall J.G. i wsp.: Elements of morphology: standard terminology for the nose and philtrum. Am. J. Med. Genet. A, 2009; 149A(1): 61–76
16. Hall B.D., Graham J.M., Cassidy S.B. i wsp.: Elements of morphology: standard terminology for the periorbital region. Am. J. Med. Genet. A, 2009; 149A (1): 29–39
17. Del Campo M., Kable J.A., Coles C.D. i wsp.: Secondary physical features in children with FASD. Eur. J. Med. Genet., 2024; 67: 104 890
18. Jacobson S.W., Hoyme H.E., Carter R.C. i wsp.: Evolution of the physical phenotype of fetal alcohol spectrum disorders from childhood through adolescence. Alcohol Clin. Exp. Res., 2021; 45 (2): 395–408
19. Fang S., McLaughlin J., Fang J. i wsp.: Automated diagnosis of fetal alcohol syndrome using 3D facial image analysis. Orthod. Craniofac. Res., 2008; 11 (3): 162–171
20. Cranston M.E., Mhanni A.A., Marles S.L. i wsp.: Concordance of three methods for palpebral fissure length measurement in the assessment of fetal alcohol spectrum disorder. Can. J. Clin. Pharmacol., 2009; 16 (1): e234–e241
21. Astley S.J.: Palpebral fissure length measurement: accuracy of the FAS facial photographic analysis software and inaccuracy of the ruler. J. Popul. Ther. Clin. Pharmacol., 2015; 22 (1): e9–e26
22. Shaner D.J., Bamforth J.S., Peterson A.E. i wsp.: Technical note: different techniques, different results – a comparison of photogrammetric and caliper-derived measurements. Am. J. Phys. Anthropol., 1998; 106 (4): 547–552
23. Jones K.L., Robinson L.K., Bakhireva L.N. i wsp.: Accuracy of the diagnosis of physical features of fetal alcohol syndrome by pediatricians after specialized training. Pediatrics, 2006; 118 (6): e1734–e1738
24. Coles C.D., Gailey A.R., Mulle J.G. i wsp.: Response to Astley’s letter to the editor. Alcohol Clin. Exp. Res., 2017; 41 (1): 219
25. Astley S.J.: https://depts.washington.edu/fasdpn/htmls/face-software.htm (dostęp: 09.04.2025)
26. Astley S.J., Clarren S.K.: Measuring the facial phenotype of individuals with prenatal alcohol exposure: correlations with brain dysfunction. Alcohol, 2001; 36 (2): 147–159
27. Strömland K., Chen Y., Norberg T. i wsp.: Reference values of facial features in Scandinavian children measured with a range-camera technique. Scand. J. Plast. Reconstr. Surg. Hand Surg., 1999; 33 (1): 59–65
28. Astley S.: FAS Diagnostic and Prevention Network. https://depts.washington.edu/fasdpn/ (dostęp: 09.04.2025)
29. Hoyme H.E., Hoyme D.B., Elliott A.J. i wsp.: A South African mixed race lip/philtrum guide for diagnosis of fetal alcohol spectrum disorders. Am. J. Med. Genet. A, 2015; 167 (4): 752–755
30. Douzgou S., Breen C., Crow Y.J. i wsp.: Diagnosing fetal alcohol syndrome: new insights from newer genetic technologies. Arch. Dis Child., 2012; 97 (9): 812–817
31. Leibson T., Neuman G., Chudley A.E. i wsp.: The differential diagnosis of fetal alcohol spectrum disorder. J. Popul. Ther. Clin. Pharmacol., 2014; 21 (1): e1–e30









